
Naloxone, sold under the brand names Narcan among others, is a medication used to reverse or reduce the effects of opioids. It is commonly used to counter decreased breathing in opioid overdose. Effects begin within two minutes when given intravenously, and within five minutes when injected into a muscle. The medicine can also be administered by spraying it into a person's nose. Naloxone commonly blocks the effects of opioids for 30 to 90 minutes. Multiple doses may be required, as the duration of action of some opioids is greater than that of naloxone.

A drug overdose is the ingestion or application of a drug or other substance in quantities much greater than are recommended. Typically it is used for cases when a risk to health will potentially result. An overdose may result in a toxic state or death.
A prescription drug is a pharmaceutical drug that legally requires a medical prescription to be dispensed. In contrast, over-the-counter drugs can be obtained without a prescription. The reason for this difference in substance control is the potential scope of misuse, from drug abuse to practicing medicine without a license and without sufficient education. Different jurisdictions have different definitions of what constitutes a prescription drug.
Opioid use disorder (OUD) is a substance use disorder characterized by cravings for opioids, continued use despite physical and/or psychological deterioration, increased tolerance with use, and withdrawal symptoms after discontinuing opioids. Opioid withdrawal symptoms include nausea, muscle aches, diarrhea, trouble sleeping, agitation, and a low mood. Addiction and dependence are important components of OUD.

Buprenorphine is an opioid used to treat opioid use disorder, acute pain, and chronic pain. It can be used under the tongue (sublingual), in the cheek (buccal), by injection, as a skin patch (transdermal), or as an implant. For opioid use disorder, it is typically started when withdrawal symptoms have begun and for the first two days of treatment under direct observation of a health-care provider. In the United States, the combination formulation of buprenorphine/naloxone (Suboxone) is usually prescribed to discourage misuse by injection. Maximum pain relief is generally within an hour with effects up to 24 hours. Buprenorphine affects different types of opioid receptors in different ways. Depending on the type of receptor, it may be an agonist, partial agonist, or antagonist. In the treatment of opioid use disorder buprenorphine is an agonist/antagonist, meaning that it relieves withdrawal symptoms from other opioids and induces some euphoria, but also blocks the ability for many other opioids, including heroin, to cause an effect. Unlike full agonists like heroin or methadone, buprenorphine has a ceiling effect, such that taking more medicine will not increase the effects of the drug.

Sufentanil, sold under the brand names Dsuvia and Sufenta, is a synthetic opioid analgesic drug approximately 5 to 10 times as potent as its parent drug, fentanyl, and 500 times as potent as morphine. Structurally, sufentanil differs from fentanyl through the addition of a methoxymethyl group on the piperidine ring, and the replacement of the phenyl ring by thiophene. Sufentanil first was synthesized at Janssen Pharmaceutica in 1974.

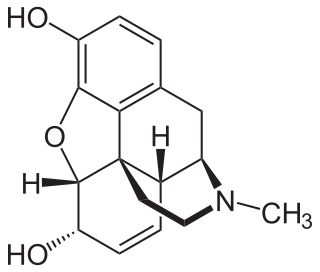
An opioid overdose is toxicity due to excessive consumption of opioids, such as morphine, codeine, heroin, fentanyl, tramadol, and methadone. This preventable pathology can be fatal if it leads to respiratory depression, a lethal condition that can cause hypoxia from slow and shallow breathing. Other symptoms include small pupils, and unconsciousness, however its onset can depend on the method of ingestion, the dosage and individual risk factors. Although there were over 110,000 deaths in 2017 due to opioids, individuals who survived also faced adverse complications, including permanent brain damage.
In the United States, prescription monitoring programs (PMPs) or prescription drug monitoring programs (PDMPs) are state-run programs which collect and distribute data about the prescription and dispensation of federally controlled substances and, depending on state requirements, other potentially abusable prescription drugs. PMPs are meant to help prevent adverse drug-related events such as opioid overdoses, drug diversion, and substance abuse by decreasing the amount and/or frequency of opioid prescribing, and by identifying those patients who are obtaining prescriptions from multiple providers or those physicians overprescribing opioids.
Buprenorphine/naloxone, sold under the brand name Suboxone among others, is a fixed-dose combination medication that includes buprenorphine and naloxone. It is used to treat opioid use disorder, and reduces the mortality of opioid use disorder by 50%. It relieves cravings to use and withdrawal symptoms. Buprenorphine/naloxone is available for use in two different forms, under the tongue or in the cheek.
The Pennsylvania Department of Drug and Alcohol Programs is a cabinet-level agency in the Government of Pennsylvania under Governor Tom Wolf. The objective of this department is to manage and distribute state and federal funds used to oversee alcohol and drug prevention, intervention and treatment services.
The California State Legislature passed an act to amend Section 1714.22 of the Civil Code, relating to drug overdose treatment in 2014. California Assembly Bill 1535 (2014) delegated the authority to all properly licensed California state pharmacists who had undergone a training program of at least one hour of continuing education about the pharmacology of naloxone hydrochloride to dispense naloxone under standards developed by the Medical Board of California in conjunction with the California Society of Addiction Medicine, the California Pharmacists Association, and any other appropriate entities.

In the United States, the opioid epidemic is an extensive ongoing overuse of opioid medications, both from medical prescriptions and from illegal sources. The epidemic began in the United States in the late 1990s, according to the Centers for Disease Control and Prevention (CDC), when opioids were increasingly prescribed for pain management and resulted in a rise in overall opioid use throughout subsequent years. The great majority of Americans who use prescription opioids do not believe that they are misusing them.

The opioid epidemic, also referred to as the opioid crisis, is the rapid increase in the overuse, misuse/abuse, and overdose deaths attributed either in part or in whole to the class of drugs opiates/opioids since the 1990s. It includes the significant medical, social, psychological, and economic consequences of the medical, non-medical, and recreational abuse of these medications.
The New Jersey “Opioid Antidote Prescription” bill is legislation sponsored in the New Jersey State Senate. The bill, numbered NJ S. 2323, requires a co-prescription of an opioid overdose agent, such as naloxone, with prescriptions for opioid medications for patients who have a high risk of overdosing and tightens restrictions on the dispensing of opioid medications in New Jersey.
The Illinois “Opioids-Covid-19-Naloxone” Resolution is legislation sponsored in the Illinois State Senate. The bill, numbered IL SR 1184, prompts the state of Illinois to examine the rise in opioid overdoses due to the COVID-19 pandemic. The bill also urges the state to improve and increase access to naloxone, an opioid overdose reversal drug.
The New York mandatory opioid antagonist prescription bill is legislation sponsored in the New York State Senate and Assembly. The Senate bill, numbered NY S. 5150-B, sponsored by state Senator Pete Harckham, will require prescribers to co-prescribe an opioid antagonist with the first opioid prescription of the year for certain high-risk patients to combat accidental overdoses.
The South Carolina opioid overdose prevention bill is legislation sponsored in the South Carolina state legislature. The bill, numbered SC H.B. 4711 and sponsored by state Representative Russell Fry, would require prescribers to offer a prescription for naloxone to patients at high risk of an opioid overdose.
The California naloxone requirement bill is legislation passed by the California legislature and signed into law in 2018. The bill, numbered AB 2760, and sponsored by state Assembly member Jim Wood, requires medical prescribers to offer a prescription for naloxone to certain populations at higher risk of overdosing from opiate drugs.
Over a period of six months, Colorado legislation HB 20–1065, the Colorado Harm Reduction Substance Use Disorders Law, passed through both houses of the state legislature with bipartisan sponsorship and was signed into law by Governor Jared Polis (D). The law provides support mechanisms and medications to individuals with substance abuse disorder. It also provides protection to pharmacists and ordinary Good Samaritans who are attempting to assist those with the potential of drug overdose and its subsequent consequences.

Prescription drug addiction is the chronic, repeated use of a prescription drug in ways other than prescribed for, including using someone else’s prescription. A prescription drug is a pharmaceutical drug that may not be dispensed without a legal medical prescription. Drugs in this category are supervised due to their potential for misuse and Substance use disorder. The classes of medications most commonly abused are opioids, central nervous system (CNS) depressants and central nervous stimulants. In particular, prescription opioid is most commonly abused in the form of prescription analgesics.