Other maternal and fetal complications (678–679)
- 678 Other fetal conditions
- 678.0 Fetal hematologic conditions
- 678.1 Fetal conjoined twins
- 679.02 Complications of in utero procedures
| Pregnancy |
| ||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Labor | |||||||||||||||||
| Puerperal | |||||||||||||||||
| Other | |||||||||||||||||
| Chapter | Block | Title |
|---|---|---|
| I | 001–139 | Infectious and Parasitic Diseases |
| II | 140–239 | Neoplasms |
| III | 240–279 | Endocrine, Nutritional and Metabolic Diseases, and Immunity Disorders |
| IV | 280–289 | Diseases of the Blood and Blood-forming Organs |
| V | 290–319 | Mental Disorders |
| VI | 320–389 | Diseases of the Nervous System and Sense Organs |
| VII | 390–459 | Diseases of the Circulatory System |
| VIII | 460–519 | Diseases of the Respiratory System |
| IX | 520–579 | Diseases of the Digestive System |
| X | 580–629 | Diseases of the Genitourinary System |
| XI | 630–679 | Complications of Pregnancy, Childbirth, and the Puerperium |
| XII | 680–709 | Diseases of the Skin and Subcutaneous Tissue |
| XIII | 710–739 | Diseases of the Musculoskeletal System and Connective Tissue |
| XIV | 740–759 | Congenital Anomalies |
| XV | 760–779 | Certain Conditions originating in the Perinatal Period |
| XVI | 780–799 | Symptoms, Signs and Ill-defined Conditions |
| XVII | 800–999 | Injury and Poisoning |
| E800–E999 | Supplementary Classification of External Causes of Injury and Poisoning | |
| V01–V82 | Supplementary Classification of Factors influencing Health Status and Contact with Health Services | |
| M8000–M9970 | Morphology of Neoplasms |
This is a shortened version of the eleventh chapter of the ICD-9: Complications of Pregnancy, Childbirth, and the Puerperium. It covers ICD codes 630 to 679. The full chapter can be found on pages 355 to 378 of Volume 1, which contains all (sub)categories of the ICD-9. Volume 2 is an alphabetical index of Volume 1. Both volumes can be downloaded for free from the website of the World Health Organization.
| Pregnancy |
| ||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Labor | |||||||||||||||||
| Puerperal | |||||||||||||||||
| Other | |||||||||||||||||
Obstetrics is the field of study concentrated on pregnancy, childbirth and the postpartum period. As a medical specialty, obstetrics is combined with gynecology under the discipline known as obstetrics and gynecology (OB/GYN), which is a surgical field.

Childbirth, also known as labour, parturition and delivery, is the completion of pregnancy where one or more babies exits the internal environment of the mother via vaginal delivery or caesarean section. In 2019, there were about 140.11 million human births globally. In the developed countries, most deliveries occur in hospitals, while in the developing countries most are home births.

Eclampsia is the onset of seizures (convulsions) in a woman with pre-eclampsia. Pre-eclampsia is a hypertensive disorder of pregnancy that presents with three main features: new onset of high blood pressure, large amounts of protein in the urine or other organ dysfunction, and edema. If left untreated, pre-eclampsia can result in long-term consequences for the mother, namely increased risk of cardiovascular diseases and associated complications. In more severe cases, it may be fatal for both the mother and the fetus. The diagnostic criteria for pre-eclampsia is high blood pressure occurring after 20 weeks gestation or during the second half of pregnancy. Most often it occurs during the 3rd trimester of pregnancy and may occur before, during, or after delivery. The seizures are of the tonic–clonic type and typically last about a minute. Following the seizure, there is either a period of confusion or coma. Other complications include aspiration pneumonia, cerebral hemorrhage, kidney failure, pulmonary edema, HELLP syndrome, coagulopathy, placental abruption and cardiac arrest.

The postpartum period begins after childbirth and is typically considered to last for six weeks. However, there are three distinct but continuous phases of the postnatal period; the acute phase, lasting for six to twelve hours after birth; the subacute phase, lasting six weeks; and the delayed phase, lasting up to six months. During the delayed phase, some changes to the genitourinary system take much longer to resolve and may result in conditions such as urinary incontinence. The World Health Organization (WHO) describes the postnatal period as the most critical and yet the most neglected phase in the lives of mothers and babies; most maternal and newborn deaths occur during this period.

Pre-eclampsia is a multi-system disorder specific to pregnancy, characterized by the onset of high blood pressure and often a significant amount of protein in the urine. When it arises, the condition begins after 20 weeks of pregnancy. In severe cases of the disease there may be red blood cell breakdown, a low blood platelet count, impaired liver function, kidney dysfunction, swelling, shortness of breath due to fluid in the lungs, or visual disturbances. Pre-eclampsia increases the risk of undesirable as well as lethal outcomes for both the mother and the fetus including preterm labor. If left untreated, it may result in seizures at which point it is known as eclampsia.

Gestational hypertension or pregnancy-induced hypertension (PIH) is the development of new hypertension in a pregnant woman after 20 weeks' gestation without the presence of protein in the urine or other signs of pre-eclampsia. Gestational hypertension is defined as having a blood pressure greater than 140/90 on two occasions at least 6 hours apart.

Placental abruption is when the placenta separates early from the uterus, in other words separates before childbirth. It occurs most commonly around 25 weeks of pregnancy. Symptoms may include vaginal bleeding, lower abdominal pain, and dangerously low blood pressure. Complications for the mother can include disseminated intravascular coagulopathy and kidney failure. Complications for the baby can include fetal distress, low birthweight, preterm delivery, and stillbirth.
Obstetrical bleeding is bleeding in pregnancy that occurs before, during, or after childbirth. Bleeding before childbirth is that which occurs after 24 weeks of pregnancy. Bleeding may be vaginal or less commonly into the abdominal cavity. Bleeding which occurs before 24 weeks is known as early pregnancy bleeding.

Shoulder dystocia is when, after vaginal delivery of the head, the baby's anterior shoulder gets caught above the mother's pubic bone. Signs include retraction of the baby's head back into the vagina, known as "turtle sign". Complications for the baby may include brachial plexus injury, or clavicle fracture. Complications for the mother may include vaginal or perineal tears, postpartum bleeding, or uterine rupture.

Complications of pregnancy are health problems that are related to, or arise during pregnancy. Complications that occur primarily during childbirth are termed obstetric labor complications, and problems that occur primarily after childbirth are termed puerperal disorders. While some complications improve or are fully resolved after pregnancy, some may lead to lasting effects, morbidity, or in the most severe cases, maternal or fetal mortality.

Uterine atony is the failure of the uterus to contract adequately following delivery. Contraction of the uterine muscles during labor compresses the blood vessels and slows flow, which helps prevent hemorrhage and facilitates coagulation. Therefore, a lack of uterine muscle contraction can lead to an acute hemorrhage, as the vasculature is not being sufficiently compressed. Uterine atony is the most common cause of postpartum hemorrhage, which is an emergency and potential cause of fatality. Across the globe, postpartum hemorrhage is among the top five causes of maternal death. Recognition of the warning signs of uterine atony in the setting of extensive postpartum bleeding should initiate interventions aimed at regaining stable uterine contraction.
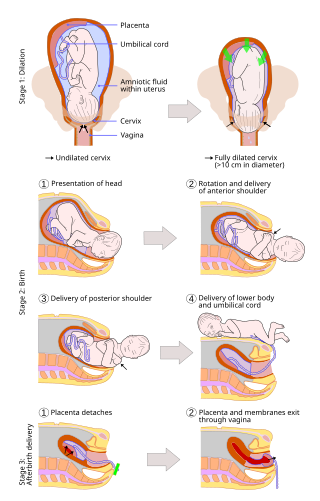
A vaginal delivery is the birth of offspring in mammals through the vagina. It is the most common method of childbirth worldwide. It is considered the preferred method of delivery, with lower morbidity and mortality than caesarean sections (C-sections).
A uterotonic, also known as an oxytocic or ecbolic, is a type of medication used to induce contraction or greater tonicity of the uterus. Uterotonics are used both to induce labor and to reduce postpartum hemorrhage.
The following outline is provided as an overview of and topical guide to obstetrics:
Psychiatric disorders of childbirth, as opposed to those of pregnancy or the postpartum period, are psychiatric complications that develop during or immediately following childbirth. Despite modern obstetrics and pain control, these disorders are still observed. Most often, psychiatric disorders of childbirth present as delirium, stupor, rage, acts of desperation, or neonaticide. These psychiatric complications are rarely seen in patients under modern medical supervision. However, care disparities between Europe, North America, Australia, Japan, and other countries with advanced medical care and the rest of the world persist. The wealthiest nations represent 10 million births each year out of the world's total of 135 million. These nations have a maternal mortality rate (MMR) of 6–20/100,000. Poorer nations with high birth rates can have an MMR more than 100 times higher. In Africa, India & South East Asia, as well as Latin America, these complications of parturition may still be as prevalent as they have been throughout human history.

Circumvallate placenta is a rare condition affecting about 1-2% of pregnancies, in which the amnion and chorion fetal membranes essentially "double back" on the fetal side around the edges of the placenta. After delivery, a circumvallate placenta has a thick ring of membranes on its fetal surface. Circumvallate placenta is a placental morphological abnormality associated with increased fetal morbidity and mortality due to the restricted availability of nutrients and oxygen to the developing fetus.
A pre-existing disease in pregnancy is a disease that is not directly caused by the pregnancy, in contrast to various complications of pregnancy, but which may become worse or be a potential risk to the pregnancy. A major component of this risk can result from necessary use of drugs in pregnancy to manage the disease.
Hypertensive disease of pregnancy, also known as maternal hypertensive disorder, is a group of high blood pressure disorders that include preeclampsia, preeclampsia superimposed on chronic hypertension, gestational hypertension, and chronic hypertension.

Emergency childbirth is the precipitous birth of an infant in an unexpected setting. In planned childbirth, mothers choose the location and obstetric team ahead of time. Options range from delivering at home, at a hospital, a medical facility or a birthing center. Sometimes, birth can occur on the way to these facilities, without a healthcare team. The rates of unplanned childbirth are low. If the birth is imminent, emergency measures may be needed. Emergency services can be contacted for help in some countries.
Maternal health outcomes differ significantly between racial groups within the United States. The American College of Obstetricians and Gynecologists describes these disparities in obstetric outcomes as "prevalent and persistent." Black, indigenous, and people of color are disproportionately affected by many of the maternal health outcomes listed as national objectives in the U.S. Department of Health and Human Services's national health objectives program, Healthy People 2030. The American Public Health Association considers maternal mortality to be a human rights issue, also noting the disparate rates of Black maternal death. Race affects maternal health throughout the pregnancy continuum, beginning prior to conception and continuing through pregnancy (antepartum), during labor and childbirth (intrapartum), and after birth (postpartum).