Related Research Articles

Hypoxia is a condition in which the body or a region of the body is deprived of adequate oxygen supply at the tissue level. Hypoxia may be classified as either generalized, affecting the whole body, or local, affecting a region of the body. Although hypoxia is often a pathological condition, variations in arterial oxygen concentrations can be part of the normal physiology, for example, during strenuous physical exercise.

The respiratory system is a biological system consisting of specific organs and structures used for gas exchange in animals and plants. The anatomy and physiology that make this happen varies greatly, depending on the size of the organism, the environment in which it lives and its evolutionary history. In land animals the respiratory surface is internalized as linings of the lungs. Gas exchange in the lungs occurs in millions of small air sacs; in mammals and reptiles these are called alveoli, and in birds they are known as atria. These microscopic air sacs have a very rich blood supply, thus bringing the air into close contact with the blood. These air sacs communicate with the external environment via a system of airways, or hollow tubes, of which the largest is the trachea, which branches in the middle of the chest into the two main bronchi. These enter the lungs where they branch into progressively narrower secondary and tertiary bronchi that branch into numerous smaller tubes, the bronchioles. In birds, the bronchioles are termed parabronchi. It is the bronchioles, or parabronchi that generally open into the microscopic alveoli in mammals and atria in birds. Air has to be pumped from the environment into the alveoli or atria by the process of breathing which involves the muscles of respiration.
Respiratory failure results from inadequate gas exchange by the respiratory system, meaning that the arterial oxygen, carbon dioxide, or both cannot be kept at normal levels. A drop in the oxygen carried in the blood is known as hypoxemia; a rise in arterial carbon dioxide levels is called hypercapnia. Respiratory failure is classified as either Type 1 or Type 2, based on whether there is a high carbon dioxide level, and can be acute or chronic. In clinical trials, the definition of respiratory failure usually includes increased respiratory rate, abnormal blood gases, and evidence of increased work of breathing. Respiratory failure causes an altered mental status due to ischemia in the brain.
Diffusing capacity of the lung (DL) measures the transfer of gas from air in the lung, to the red blood cells in lung blood vessels. It is part of a comprehensive series of pulmonary function tests to determine the overall ability of the lung to transport gas into and out of the blood. DL, especially DLCO, is reduced in certain diseases of the lung and heart. DLCO measurement has been standardized according to a position paper by a task force of the European Respiratory and American Thoracic Societies.
Dead space is the volume of air that is inhaled that does not take part in the gas exchange, because it either remains in the conducting airways or reaches alveoli that are not perfused or poorly perfused. It means that not all the air in each breath is available for the exchange of oxygen and carbon dioxide. Mammals breathe in and out of their lungs, wasting that part of the inhalation which remains in the conducting airways where no gas exchange can occur.

Gas exchange is the physical process by which gases move passively by diffusion across a surface. For example, this surface might be the air/water interface of a water body, the surface of a gas bubble in a liquid, a gas-permeable membrane, or a biological membrane that forms the boundary between an organism and its extracellular environment.

Acute respiratory distress syndrome (ARDS) is a type of respiratory failure characterized by rapid onset of widespread inflammation in the lungs. Symptoms include shortness of breath (dyspnea), rapid breathing (tachypnea), and bluish skin coloration (cyanosis). For those who survive, a decreased quality of life is common.
In physiology, respiration is the movement of oxygen from the outside environment to the cells within tissues, and the removal of carbon dioxide in the opposite direction that's to the environment.

Respiratory acidosis is a state in which decreased ventilation (hypoventilation) increases the concentration of carbon dioxide in the blood and decreases the blood's pH.

Hypoxemia is an abnormally low level of oxygen in the blood. More specifically, it is oxygen deficiency in arterial blood. Hypoxemia has many causes, and often causes hypoxia as the blood is not supplying enough oxygen to the tissues of the body.
A pulmonary shunt is the passage of deoxygenated blood from the right side of the heart to the left without participation in gas exchange in the pulmonary capillaries. It is a pathological condition that results when the alveoli of parts of the lungs are perfused with blood as normal, but ventilation fails to supply the perfused region. In other words, the ventilation/perfusion ratio of those areas is zero.
The zones of the lung divide the lung into four vertical regions, based upon the relationship between the pressure in the alveoli (PA), in the arteries (Pa), in the veins (Pv) and the pulmonary interstitial pressure (Pi):
The factors that determine the values for alveolar pO2 and pCO2 are:
The alveolar gas equation is the method for calculating partial pressure of alveolar oxygen (PAO2). The equation is used in assessing if the lungs are properly transferring oxygen into the blood. The alveolar air equation is not widely used in clinical medicine, probably because of the complicated appearance of its classic forms. The partial pressure of oxygen (pO2) in the pulmonary alveoli is required to calculate both the alveolar-arterial gradient of oxygen and the amount of right-to-left cardiac shunt, which are both clinically useful quantities. However, it is not practical to take a sample of gas from the alveoli in order to directly measure the partial pressure of oxygen. The alveolar gas equation allows the calculation of the alveolar partial pressure of oxygen from data that is practically measurable. It was first characterized in 1946.
The multiple inert gas elimination technique (MIGET) is a medical technique used mainly in pulmonology that involves measuring the concentrations of various infused, inert gases in mixed venous blood, arterial blood, and expired gas of a subject. The technique quantifies true shunt, physiological dead space ventilation, ventilation versus blood flow ratios, and diffusion limitation.
The Alveolar–arterial gradient, is a measure of the difference between the alveolar concentration (A) of oxygen and the arterial (a) concentration of oxygen. It is a useful parameter for narrowing the differential diagnosis of hypoxemia.
Fraction of inspired oxygen (FIO2), correctly denoted with a capital I, is the molar or volumetric fraction of oxygen in the inhaled gas. Medical patients experiencing difficulty breathing are provided with oxygen-enriched air, which means a higher-than-atmospheric FIO2. Natural air includes 21% oxygen, which is equivalent to FIO2 of 0.21. Oxygen-enriched air has a higher FIO2 than 0.21; up to 1.00 which means 100% oxygen. FIO2 is typically maintained below 0.5 even with mechanical ventilation, to avoid oxygen toxicity, but there are applications when up to 100% is routinely used.
In the respiratory system, ventilation/perfusion (V/Q) mismatch refers to the pathological discrepancy between ventilation (V) and perfusion (Q) resulting in an abnormal ventilation/perfusion (V/Q) ratio. Ventilation is a measure of the amount of inhaled air that reaches the alveoli, while perfusion is a measure of the amount of deoxygenated blood that reaches the alveoli through the capillary beds. Under normal conditions, ventilation-perfusion coupling keeps ventilation (V) at approximately 4 L/min and normal perfusion (Q) at approximately 5 L/min. Thus, at rest, a normal V/Q ratio is 0.8. Any deviation from this value is considered a V/Q mismatch. Maintenance of the V/Q ratio is crucial for preservation of effective pulmonary gas exchange and maintenance of oxygenation levels. A mismatch can contribute to hypoxemia and often signifies the presence or worsening of an underlying pulmonary condition.
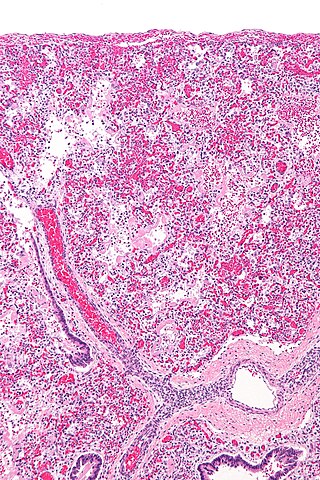
The pathophysiology of acute respiratory distress syndrome involves fluid accumulation in the lungs not explained by heart failure. It is typically provoked by an acute injury to the lungs that results in flooding of the lungs' microscopic air sacs responsible for the exchange of gases such as oxygen and carbon dioxide with capillaries in the lungs. Additional common findings in ARDS include partial collapse of the lungs (atelectasis) and low levels of oxygen in the blood (hypoxemia). The clinical syndrome is associated with pathological findings including pneumonia, eosinophilic pneumonia, cryptogenic organizing pneumonia, acute fibrinous organizing pneumonia, and diffuse alveolar damage (DAD). Of these, the pathology most commonly associated with ARDS is DAD, which is characterized by a diffuse inflammation of lung tissue. The triggering insult to the tissue usually results in an initial release of chemical signals and other inflammatory mediators secreted by local epithelial and endothelial cells.

Ventilation-perfusion coupling is the relationship between ventilation and perfusion processes, which take place in the respiratory system and the cardiovascular system. Ventilation is the movement of gas during breathing, and perfusion is the process of pulmonary blood circulation, which delivers oxygen to body tissues. Anatomically, the lung structure, alveolar organization, and alveolar capillaries contribute to the physiological mechanism of ventilation and perfusion. Ventilation-perfusion coupling maintains a constant ventilation/perfusion ratio near 0.8 on average, while the regional variation exists within the lungs due to gravity. When the ratio gets above or below 0.8, it is considered abnormal ventilation-perfusion coupling, also known as a ventilation–perfusion mismatch. Lung diseases, cardiac shunts, and smoking can cause a ventilation-perfusion mismatch that results in significant symptoms and diseases, which can be treated through treatments like bronchodilators and oxygen therapy.
References
- ↑ Derenoncourt, Paul-Robert; Felder, Gabriel J.; Royal, Henry D.; Bhalla, Sanjeev; Lang, Jordan A.; Matesan, Manuela C.; Itani, Malak (November 2021). "Ventilation-Perfusion Scan: A Primer for Practicing Radiologists". RadioGraphics. 41 (7): 2047–2070. doi:10.1148/rg.2021210060. ISSN 0271-5333.
- ↑ Mirza, Hasan; Hashmi, Muhammad F. (2023), "Lung Ventilation Perfusion Scan (VQ Scan)", StatPearls, Treasure Island (FL): StatPearls Publishing, PMID 33232086 , retrieved 2023-11-12
- ↑ Roach, Paul J.; Schembri, Geoffrey P.; Bailey, Dale L. (2013-09-01). "V/Q Scanning Using SPECT and SPECT/CT". Journal of Nuclear Medicine. 54 (9): 1588–1596. doi: 10.2967/jnumed.113.124602 . ISSN 0161-5505. PMID 23907760.
- ↑ VQ Ratio
- ↑ Physiology of capnography
- ↑ "Respiratory Physiology (page 2)". Archived from the original on 2006-12-11. Retrieved 2006-12-17.