
The sense of balance or equilibrioception is the perception of balance and spatial orientation. It helps prevent humans and nonhuman animals from falling over when standing or moving. Equilibrioception is the result of a number of sensory systems working together; the eyes, the inner ears, and the body's sense of where it is in space (proprioception) ideally need to be intact.
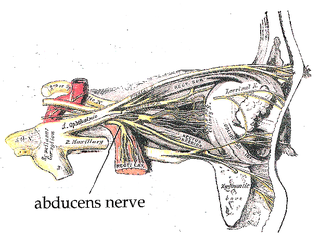
The abducens nerve or abducent nerve, also known as the sixth cranial nerve, cranial nerve VI, or simply CN VI, is a cranial nerve in humans and various other animals that controls the movement of the lateral rectus muscle, one of the extraocular muscles responsible for outward gaze. It is a somatic efferent nerve.
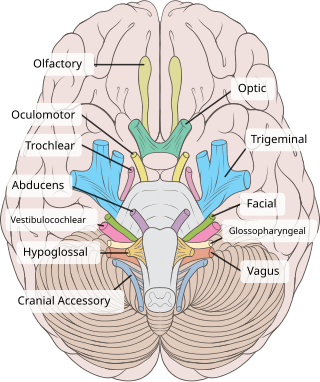
The oculomotor nerve, also known as the third cranial nerve, cranial nerve III, or simply CN III, is a cranial nerve that enters the orbit through the superior orbital fissure and innervates extraocular muscles that enable most movements of the eye and that raise the eyelid. The nerve also contains fibers that innervate the intrinsic eye muscles that enable pupillary constriction and accommodation. The oculomotor nerve is derived from the basal plate of the embryonic midbrain. Cranial nerves IV and VI also participate in control of eye movement.

The vestibular system, in vertebrates, is a sensory system that creates the sense of balance and spatial orientation for the purpose of coordinating movement with balance. Together with the cochlea, a part of the auditory system, it constitutes the labyrinth of the inner ear in most mammals.
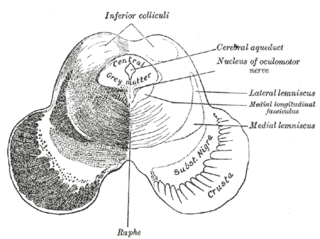
The medial longitudinal fasciculus (MLF) is an area of crossed over tracts, on each side of the brainstem. These bundles of axons are situated near the midline of the brainstem. They are made up of both ascending and descending fibers that arise from a number of sources and terminate in different areas, including the superior colliculus, the vestibular nuclei, and the cerebellum. It contains the interstitial nucleus of Cajal, responsible for oculomotor control, head posture, and vertical eye movement.

The accommodation reflex is a reflex action of the eye, in response to focusing on a near object, then looking at a distant object, comprising coordinated changes in vergence, lens shape (accommodation) and pupil size. It is dependent on cranial nerve II, superior centers (interneuron) and cranial nerve III. The change in the shape of the lens is controlled by ciliary muscles inside the eye. Changes in contraction of the ciliary muscles alter the focal distance of the eye, causing nearer or farther images to come into focus on the retina; this process is known as accommodation. The reflex, controlled by the parasympathetic nervous system, involves three responses: pupil constriction, lens accommodation, and convergence.

Eye movement includes the voluntary or involuntary movement of the eyes. Eye movements are used by a number of organisms to fixate, inspect and track visual objects of interests. A special type of eye movement, rapid eye movement, occurs during REM sleep.
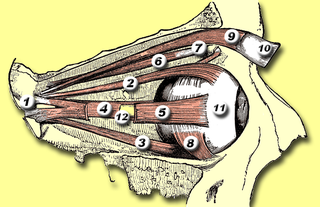
The medial rectus muscle is a muscle in the orbit near the eye. It is one of the extraocular muscles. It originates from the common tendinous ring, and inserts into the anteromedial surface of the eye. It is supplied by the inferior division of the oculomotor nerve (III). It rotates the eye medially (adduction).

The extraocular muscles, or extrinsic ocular muscles, are the seven extrinsic muscles of the human eye. Six of the extraocular muscles, the four recti muscles, and the superior and inferior oblique muscles, control movement of the eye and the other muscle, the levator palpebrae superioris, controls eyelid elevation. The actions of the six muscles responsible for eye movement depend on the position of the eye at the time of muscle contraction.
Oscillopsia is a visual disturbance in which objects in the visual field appear to oscillate. The severity of the effect may range from a mild blurring to rapid and periodic jumping. Oscillopsia is an incapacitating condition experienced by many patients with neurological disorders. It may be the result of ocular instability occurring after the oculomotor system is affected, no longer holding images steady on the retina. A change in the magnitude of the vestibulo-ocular reflex due to vestibular disease can also lead to oscillopsia during rapid head movements. Oscillopsia may also be caused by involuntary eye movements such as nystagmus, or impaired coordination in the visual cortex and is one of the symptoms of superior canal dehiscence syndrome. Those affected may experience dizziness and nausea. Oscillopsia can also be used as a quantitative test to document aminoglycoside toxicity. Permanent oscillopsia can arise from an impairment of the ocular system that serves to maintain ocular stability. Paroxysmal oscillopsia can be due to an abnormal hyperactivity in the peripheral ocular or vestibular system.

The abducens nucleus is the originating nucleus from which the abducens nerve (VI) emerges—a cranial nerve nucleus. This nucleus is located beneath the fourth ventricle in the caudal portion of the pons near the midline, medial to the sulcus limitans.

The flocculus is a small lobe of the cerebellum at the posterior border of the middle cerebellar peduncle anterior to the biventer lobule. Like other parts of the cerebellum, the flocculus is involved in motor control. It is an essential part of the vestibulo-ocular reflex, and aids in the learning of basic motor skills in the brain.

In medicine, the caloric reflex test is a test of the vestibulo-ocular reflex that involves irrigating cold or warm water or air into the external auditory canal. This method was developed by Robert Bárány, who won a Nobel prize in 1914 for this discovery.

The vestibulospinal tract is a neural tract in the central nervous system. Specifically, it is a component of the extrapyramidal system and is classified as a component of the medial pathway. Like other descending motor pathways, the vestibulospinal fibers of the tract relay information from nuclei to motor neurons. The vestibular nuclei receive information through the vestibulocochlear nerve about changes in the orientation of the head. The nuclei relay motor commands through the vestibulospinal tract. The function of these motor commands is to alter muscle tone, extend, and change the position of the limbs and head with the goal of supporting posture and maintaining balance of the body and head.

The cranial nerve exam is a type of neurological examination. It is used to identify problems with the cranial nerves by physical examination. It has nine components. Each test is designed to assess the status of one or more of the twelve cranial nerves (I-XII). These components correspond to testing the sense of smell (I), visual fields and acuity (II), eye movements and pupils, sensory function of face (V), strength of facial (VII) and shoulder girdle muscles (XI), hearing and balance, taste, pharyngeal movement and reflex, tongue movements (XII).
Conjugate gaze palsies are neurological disorders affecting the ability to move both eyes in the same direction. These palsies can affect gaze in a horizontal, upward, or downward direction. These entities overlap with ophthalmoparesis and ophthalmoplegia.
Listing's law, named after German mathematician Johann Benedict Listing (1808–1882), describes the three-dimensional orientation of the eye and its axes of rotation. Listing's law has been shown to hold when the head is stationary and upright and gaze is directed toward far targets, i.e., when the eyes are either fixating, making saccades, or pursuing moving visual targets.
The term gaze is frequently used in physiology to describe coordinated motion of the eyes and neck. The lateral gaze is controlled by the paramedian pontine reticular formation (PPRF). The vertical gaze is controlled by the rostral interstitial nucleus of medial longitudinal fasciculus and the interstitial nucleus of Cajal.
The righting reflex, also known as the labyrinthine righting reflex, is a reflex that corrects the orientation of the body when it is taken out of its normal upright position. It is initiated by the vestibular system, which detects that the body is not erect and causes the head to move back into position as the rest of the body follows. The perception of head movement involves the body sensing linear acceleration or the force of gravity through the otoliths, and angular acceleration through the semicircular canals. The reflex uses a combination of visual system inputs, vestibular inputs, and somatosensory inputs to make postural adjustments when the body becomes displaced from its normal vertical position. These inputs are used to create what is called an efference copy. This means that the brain makes comparisons in the cerebellum between expected posture and perceived posture, and corrects for the difference. The reflex takes 6 or 7 weeks to perfect, but can be affected by various types of balance disorders.
In neuroanatomy, corticomesencephalic tract is a descending nerve tract that originates in the frontal eye field and terminate in the midbrain. Its fibers mediate conjugate eye movement.

{kind=link}