
The iliohypogastric nerve is a nerve that originates from the lumbar plexus that supplies sensation to skin over the lateral gluteal region and motor to the internal and transverse abdominal muscles.
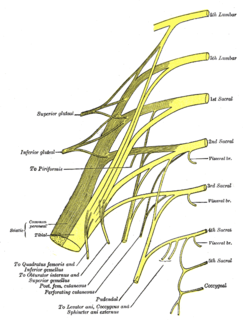
The perforating cutaneous nerve is a cutaneous nerve that supplies skin over the gluteus maximus muscle.

The zygomaticofacial nerve or zygomaticofacial branch of zygomatic nerve passes along the infero-lateral angle of the orbit, emerges upon the face through the zygomaticofacial foramen in the zygomatic bone, and, perforating the orbicularis oculi to reach the skin of the malar area.

The posterior cutaneous nerve of forearm is a nerve found in humans and other animals. It is also known as the dorsal antebrachial cutaneous nerve, the external cutaneous branch of the musculospiral nerve, and the posterior antebrachial cutaneous nerve. It is a cutaneous nerve of the forearm.

The dorsal branch of ulnar nerve arises about 5 cm. proximal to the wrist; it passes backward beneath the Flexor carpi ulnaris, perforates the deep fascia, and, running along the ulnar side of the back of the wrist and hand, divides into two dorsal digital branches; one supplies the ulnar side of the little finger; the other, the adjacent sides of the little and ring fingers.

The anterior divisions of the seventh, eighth, ninth, tenth, and eleventh thoracic intercostal nerves are continued anteriorly from the intercostal spaces into the abdominal wall; hence they are named thoraco-abdominal nerves.

The anterior cutaneous branches of the femoral nerve consist of the following nerves: intermediate cutaneous nerve and medial cutaneous nerve.

The medial calcaneal branches of the tibial nerve perforate the laciniate ligament, and supply the skin of the heel and medial side of the sole of the foot.
Cutaneous innervation refers to the area of the skin which is supplied by a specific nerve.

Blue nevus is a type of melanocytic nevus. The blue colour is caused by the pigment being deeper in the skin than in ordinary nevi. In principle they are harmless but they can sometimes be mimicked by malignant lesions, i.e. some melanomas can look like a blue nevus.

Elastosis perforans serpiginosa is a unique perforating disorder characterized by transepidermal elimination of elastic fibers and distinctive clinical lesions, which are serpiginous in distribution and can be associated with specific diseases.
Reactive perforating collagenosis is a rare, familial, nonpuritic skin disorder characterized by papules that grow in a diameter of 4 to 6mm and develop a central area of umbilication to which keratinous material is lodged. The cause of reactive perforating collagenosis is unknown.
Perforating calcific elastosis is an acquired, localized cutaneous disorder, most frequently found in obese, multiparous, middle-aged women, characterized by lax, well-circumscribed, reticulated or cobble-stoned plaques occurring in the periumbilical region with keratotic surface papules.
Verrucous perforating collagenoma is a very rare skin disorder which presents with verrucous papules with a transepidermal elimination of collagen.
The perforating branches of the internal thoracic artery pierce through the internal intercostal muscles of the superior six intercostal spaces. These small arteries run with the anterior cutaneous branches of the intercostal nerves.
Perforator flap surgery is a technique used in reconstructive surgery where skin and/or subcutaneous fat are removed from a distant or adjacent part of the body to reconstruct the excised part. The vessels that supply blood to the flap are isolated perforator(s) derived from a deep vascular system through the underlying muscle or intermuscular septa. Some perforators can have a mixed septal and intramuscular course before reaching the skin. The name of the particular flap is retrieved from its perforator and not from the underlying muscle. If there is a potential to harvest multiple perforator flaps from one vessel, the name of each flap is based on its anatomical region or muscle. For example, a perforator that only traverses through the septum to supply the underlying skin is called a septal perforator. Whereas a flap that is vascularised by a perforator traversing only through muscle to supply the underlying skin is called a muscle perforator. According to the distinct origin of their vascular supply, perforators can be classified into direct and indirect perforators. Direct perforators only pierce the deep fascia, they don't traverse any other structural tissue. Indirect perforators first run through other structures before piercing the deep fascia.
Sarcoidosis involves the skin in about 25% of patients. The most common lesions are erythema nodosum, plaques, maculopapular eruptions, subcutaneous nodules, and lupus pernio. Treatment is not required, since the lesions usually resolve spontaneously in two to four weeks. Although it may be disfiguring, cutaneous sarcoidosis rarely causes major problems.