
Gastroenterology is the branch of medicine focused on the digestive system and its disorders. The digestive system consists of the gastrointestinal tract, sometimes referred to as the GI tract, which includes the esophagus, stomach, small intestine and large intestine as well as the accessory organs of digestion which include the pancreas, gallbladder, and liver.

An endoscopy is a procedure used in medicine to look inside the body. The endoscopy procedure uses an endoscope to examine the interior of a hollow organ or cavity of the body. Unlike many other medical imaging techniques, endoscopes are inserted directly into the organ.

Colonoscopy or coloscopy is a medical procedure involving the endoscopic examination of the large bowel (colon) and the distal portion of the small bowel. This examination is performed using either a CCD camera or a fiber optic camera, which is mounted on a flexible tube and passed through the anus.

Fecal occult blood (FOB) refers to blood in the feces that is not visibly apparent. A fecal occult blood test (FOBT) checks for hidden (occult) blood in the stool (feces).

In medicine (gastroenterology), angiodysplasia is a small vascular malformation of the gut. It is a common cause of otherwise unexplained gastrointestinal bleeding and anemia. Lesions are often multiple, and frequently involve the cecum or ascending colon, although they can occur at other places. Treatment may be with colonoscopic interventions, angiography and embolization, medication, or occasionally surgery.
Gastrointestinal bleeding, also called gastrointestinal hemorrhage (GIB), is all forms of bleeding in the gastrointestinal tract, from the mouth to the rectum. When there is significant blood loss over a short time, symptoms may include vomiting red blood, vomiting black blood, bloody stool, or black stool. Small amounts of bleeding over a long time may cause iron-deficiency anemia resulting in feeling tired or heart-related chest pain. Other symptoms may include abdominal pain, shortness of breath, pale skin, or passing out. Sometimes in those with small amounts of bleeding no symptoms may be present.
Blood in stool or rectal bleeding looks different depending on how early it enters the digestive tract—and thus how much digestive action it has been exposed to—and how much there is. The term can refer either to melena, with a black appearance, typically originating from upper gastrointestinal bleeding; or to hematochezia, with a red color, typically originating from lower gastrointestinal bleeding. Evaluation of the blood found in stool depends on its characteristics, in terms of color, quantity and other features, which can point to its source, however, more serious conditions can present with a mixed picture, or with the form of bleeding that is found in another section of the tract. The term "blood in stool" is usually only used to describe visible blood, and not fecal occult blood, which is found only after physical examination and chemical laboratory testing.
Rectal bleeding refers to bleeding in the rectum. There are many causes of rectal hemorrhage, including inflamed hemorrhoids, rectal varices, proctitis, stercoral ulcers and infections. Diagnosis is usually made by proctoscopy, which is an endoscopic test.

Ischemic colitis is a medical condition in which inflammation and injury of the large intestine result from inadequate blood supply. Although uncommon in the general population, ischemic colitis occurs with greater frequency in the elderly, and is the most common form of bowel ischemia. Causes of the reduced blood flow can include changes in the systemic circulation or local factors such as constriction of blood vessels or a blood clot. In most cases, no specific cause can be identified.

Double-balloon enteroscopy, also known as push-and-pull enteroscopy, is an endoscopic technique for visualization of the small bowel. It was developed by Hironori Yamamoto in 2001. It is novel in the field of diagnostic gastroenterology as it is the first endoscopic technique that allows for the entire gastrointestinal tract to be visualized in real time.

Hemosuccus pancreaticus is a rare cause of hemorrhage in the gastrointestinal tract. It is caused by a bleeding source in the pancreas, pancreatic duct, or structures adjacent to the pancreas, such as the splenic artery, that bleed into the pancreatic duct, which is connected with the bowel at the duodenum, the first part of the small intestine. Patients with hemosuccus may develop symptoms of gastrointestinal hemorrhage, such as blood in the stools, maroon stools, or melena, which is a dark, tarry stool caused by digestion of red blood cells. They may also develop abdominal pain. It is associated with pancreatitis, pancreatic cancer and aneurysms of the splenic artery. Hemosuccus may be identified with endoscopy (esophagogastroduodenoscopy), where fresh blood may be seen from the pancreatic duct. Alternatively, angiography may be used to inject the celiac axis to determine the blood vessel that is bleeding. This may also be used to treat hemosuccus, as embolization of the end vessel may terminate the hemorrhage. However, a distal pancreatectomy—surgery to remove of the tail of the pancreas—may be required to stop the hemorrhage.
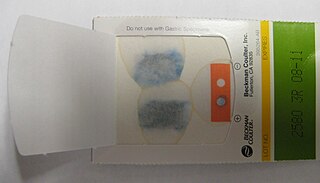
The stool guaiac test or guaiac fecal occult blood test (gFOBT) is one of several methods that detects the presence of fecal occult blood. The test involves placing a fecal sample on guaiac paper and applying hydrogen peroxide which, in the presence of blood, yields a blue reaction product within seconds.

Intestinal ischemia is a medical condition in which injury to the large or small intestine occurs due to not enough blood supply. It can come on suddenly, known as acute intestinal ischemia, or gradually, known as chronic intestinal ischemia. The acute form of the disease often presents with sudden severe abdominal pain and is associated with a high risk of death. The chronic form typically presents more gradually with abdominal pain after eating, unintentional weight loss, vomiting, and fear of eating.

An endoclip is a metallic mechanical device used in endoscopy in order to close two mucosal surfaces without the need for surgery and suturing. Its function is similar to a suture in gross surgical applications, as it is used to join together two disjointed surfaces, but, can be applied through the channel of an endoscope under direct visualization. Endoclips have found use in treating gastrointestinal bleeding, in preventing bleeding after therapeutic procedures such as polypectomy, and in closing gastrointestinal perforations. Many forms of endoclips exist of different shapes and sizes, including two and three prong devices, which can be administered using single use and reloadable systems, and may or may not open and close to facilitate placement.

Capsule endoscopy is a medical procedure used to record internal images of the gastrointestinal tract for use in disease diagnosis. Newer developments are also able to take biopsies and release medication at specific locations of the entire gastrointestinal tract. Unlike the more widely used endoscope, capsule endoscopy provides the ability to see the middle portion of the small intestine. It can be applied to the detection of various gastrointestinal cancers, digestive diseases, ulcers, unexplained bleedings, and general abdominal pains. After a patient swallows the capsule, it passes along the gastrointestinal tract, taking a number of images per second which are transmitted wirelessly to an array of receivers connected to a portable recording device carried by the patient. General advantages of capsule endoscopy over standard endoscopy include the minimally invasive procedure setup, ability to visualize more of the gastrointestinal tract, and lower cost of the procedure.
Therapeutic endoscopy is the medical term for an endoscopic procedure during which treatment is carried out via the endoscope. This contrasts with diagnostic endoscopy, where the aim of the procedure is purely to visualize a part of the gastrointestinal, respiratory or urinary tract in order to aid diagnosis. In practice, a procedure which starts as a diagnostic endoscopy may become a therapeutic endoscopy depending on the findings, such as in cases of upper gastrointestinal bleeding, or the finding of polyps during colonoscopy.

An endoscopy unit refers to a dedicated area where medical procedures are performed with endoscopes, which are cameras used to visualize structures within the body, such as the digestive tract and genitourinary system. Endoscopy units may be located within a hospital, incorporated within other medical care centres, or may be stand-alone in nature.

Herpes esophagitis is a viral infection of the esophagus caused by Herpes simplex virus (HSV).

Chromoendoscopy is a medical procedure wherein dyes are instilled into the gastrointestinal tract at the time of visualization with fibre-optic endoscopy. The purposes of chromoendoscopy is chiefly enhance the characterization of tissues, although dyes may be used for other functional purposes. The detail achieved with chromoendoscopy can often allow for identification of the tissue type or pathology based upon the pattern uncovered.

Colonic ulcer can occur at any age, in children however they are rare. Most common symptoms are abdominal pain and hematochezia.