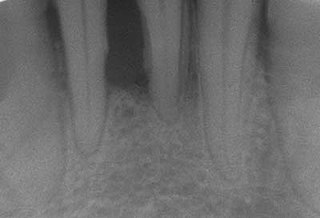
Heavy staining and calculus deposits exhibited on the lingual surface of the mandibularanterior teeth, along the gumlineCalculus deposit (indicated with a red arrow) on x-ray image
In dentistry, calculus or tartar is a form of hardened dental plaque. It is caused by precipitation of minerals from saliva and gingival crevicular fluid (GCF) in plaque on the teeth. This process of precipitation kills the bacterial cells within dental plaque, but the rough and hardened surface that is formed provides an ideal surface for further plaque formation. This leads to calculus buildup, which compromises the health of the gingiva (gums). Calculus can form both along the gumline, where it is referred to as supragingival ("above the gum"), and within the narrow sulcus that exists between the teeth and the gingiva, where it is referred to as subgingival ("below the gum").
Calculus formation is associated with a number of clinical manifestations, including bad breath, receding gums and chronically inflamed gingiva. Brushing and flossing can remove plaque from which calculus forms; however, once formed, calculus is too hard (firmly attached) to be removed with a toothbrush. Calculus buildup can be removed with ultrasonic tools or dental hand instruments (such as a periodontal scaler).
Etymology
The word comes from Latin calculus "small stone", from calx "limestone, lime",[1] probably related to Greek χάλιξchalix "small stone, pebble, rubble",[2] which many[who?] trace to a Proto-Indo-European root for "split, break up".[3]Calculus was a term used for various kinds of stones. This spun off many modern words, including "calculate" (use stones for mathematical purposes), and "calculus", which came to be used, in the 18th century, for accidental or incidental mineral buildups in human and animal bodies, like kidney stones and minerals on teeth.[3]
Tartar, on the other hand, originates in Greek as well (tartaron), but as the term for the white encrustation inside casks (a.k.a. potassium bitartrate, commonly known as cream of tartar). This came to be a term used for calcium phosphate on teeth in the early 19th century.[4]
Chemical composition
Calculus is composed of both inorganic (mineral) and organic (cellular and extracellular matrix) components.
In supra-gingival calculus
The mineral proportion of supragingival calculus ranges from approximately 40–60%, depending on its location in the dentition,[5] and consists primarily of calcium phosphate crystals organized into four principal mineral phases, listed here in order of decreasing ratio of phosphate to calcium:
The organic component is approximately 85% cellular and 15% extracellular matrix.[5] Cell density within dental plaque and calculus is very high, consisting of an estimated 200,000,000 cells per milligram.[6][7] The cells within calculus are primarily bacterial, but also include at least one species of archaea (Methanobrevibacter oralis) and several species of yeast (e.g., Candida albicans). The organic extracellular matrix in calculus consists primarily of proteins and lipids (fatty acids, triglycerides, glycolipids, and phospholipids),[5] as well as extracellular DNA.[6][8] Trace amounts of host, dietary, and environmental microdebris are also found within calculus, including salivary proteins,[9] plant DNA,[10] milk proteins,[11] starch granules,[12] textile fibers,[13] and smoke particles.[14]
In sub-gingival calculus
Sub-gingival calculus is composed almost entirely of two components: fossilized anaerobic bacteria whose biological composition has been replaced by calcium phosphate salts, and calcium phosphate salts that have joined the fossilized bacteria in calculus formations.[15]
The following minerals are detectable in calculus by X-ray diffraction:
carbonate-containing hydroxyapatite (approximately Ca5(PO4)3OH but containing some carbonate).[16]
Calculus formation
Dental calculus typically forms in incremental layers[17] that are easily visible using both electron microscopy and light microscopy.[9] These layers form during periodic calcification events of the dental plaque,[18] but the timing and triggers of these events are not well understood. The formation of calculus varies widely among individuals and at different locations within the mouth. Many variables have been identified that influence the formation of dental calculus, including age, sex, ethnic background, diet, location in the oral cavity, oral hygiene, bacterial plaque composition, host genetics, access to professional dental care, physical disabilities, systemic diseases, tobacco use, and drugs and medications.[18]
Supragingival calculus formation is most abundant on the buccal (cheek) surfaces of the maxillary (upper jaw)molars and on the lingual (tongue) surfaces of the mandibular (lower jaw) incisors.[18] These areas experience high salivary flow because of their proximity to the parotid and sublingual salivary glands.
Subgingival calculus forms below the gumline and is typically darkened in color by the presence of black-pigmented bacteria,[18] whose cells are coated in a layer of iron obtained from heme during gingival bleeding.[19] The reason fossilized bacteria are initially attracted to one part of the subgingival tooth surface over another is not fully understood. However, once the first layer is attached, more calculus components are naturally attracted to the same places due to electrical charge. This is because the calcium phosphate salts contained in them exist as electrically unstable ions (unlike calcium phosphate, the primary component of teeth). The fossilized bacteria pile up rather haphazardly, while free-floating ionic components (calcium phosphate salts) fill in the gaps.[15]
The resultant hardened structure can be compared to concrete; with the fossilized bacteria playing the role of aggregate, and the smaller calcium phosphate salts being the cement. The "hardened" calculus formations are at the heart of periodontal disease and treatment.[15]
Clinical significance
Retentive surface of calculus allows for further plaque accumulation.
Plaque accumulation causes the gingiva to become irritated and inflamed, and this is referred to as gingivitis. When the gingiva become so irritated that there is a loss of the connective tissuefibers that attach the gums to the teeth and bone that surrounds the tooth, this is known as periodontitis. Dental plaque is not the sole cause of periodontitis; however it is many times referred to as a primary aetiology. Plaque that remains in the oral cavity long enough will eventually calcify and become calculus.[18] Calculus is detrimental to gingival health because it serves as a trap for increased plaque formation and retention; thus, calculus, along with other factors that cause a localized build-up of plaque, is referred to as a secondary aetiology of periodontitis.
When plaque is supragingival, the bacterial content contains a great proportion of aerobic bacteria and yeast,[20] or those bacteria which utilize and can survive in an environment containing oxygen. Subgingival plaque contains a higher proportion of anaerobic bacteria, or those bacteria which cannot exist in an environment containing oxygen. Several anaerobic plaque bacteria, such as Porphyromonas gingivalis,[21] secrete antigenic proteins that trigger a strong inflammatory response in the periodontium, the specialized tissues that surround and support the teeth. Prolonged inflammation of the periodontium leads to bone loss and weakening of the gingival fibers that attach the teeth to the gums, two major hallmarks of periodontitis. Supragingival calculus formation is nearly ubiquitous in humans,[22][23][24] but to differing degrees. Almost all individuals with periodontitis exhibit considerable subgingival calculus deposits.[18] Dental plaque bacteria have been linked to cardiovascular disease[25] and mothers giving birth to pre-term low weight infants,[26] but there is no conclusive evidence yet that periodontitis is a significant risk factor for either of these two conditions.[27]
Prevention
Toothpaste with pyrophosphates or zinc citrate has been shown to produce a statistically significant reduction in plaque accumulation, but the effect of zinc citrate is so modest that its clinical importance is questionable.[28][29] Some calculus may form even without plaque deposits, by direct mineralisation of the pellicle.
Calculus in other animals
Calculus formation in other animals is less well studied than in humans, but it is known to form in a wide range of species. Domestic pets, such as dogs and cats, frequently accumulate large calculus deposits.[30] Animals with highly abrasive diets, such as ruminants and equids, rarely form thick deposits and instead tend to form thin calculus deposits that often have a metallic or opalescent sheen.[31] In animals, calculus should not be confused with crown cementum,[32] a layer of calcified dental tissue that encases the tooth root underneath the gingival margin and is gradually lost through periodontal disease.
Archaeological significance
Dental calculus has been shown to contain well preserved microparticles, DNA and protein in archaeological samples.[33][34] The information these molecules contain can reveal information about the oral microbiome of the host and the presence of pathogens.[35] It is also possible to identify dietary sources[36] as well as study dietary shifts[37] and occasionally evidence of craft activities.[38]
Plaque and calculus deposits are a major etiological factor in the development and progression of oral disease. An important part of the scope of practice of a dental hygienist is the removal of plaque and calculus deposits. This is achieved through the use of specifically designed instruments for debridement of tooth surfaces.[39][40] Treatment with these types of instruments is necessary as calculus deposits cannot be removed by brushing or flossing alone. To effectively manage disease or maintain oral health, thorough removal of calculus deposits should be completed at frequent intervals. The recommended frequency of dental hygiene treatment can be made by a registered professional, and is dependent on individual patient needs.[41] Factors that are taken into consideration include an individual's overall health status, tobacco use, amount of calculus present, and adherence to a professionally recommended home care routine.[42]
Hand instruments are specially designed tools used by dental professionals to remove plaque and calculus deposits that have formed on the teeth.[39][40] These tools include scalers, curettes, jaquettes, hoes, files and chisels.[39][40] Each type of tool is designed to be used in specific areas of the mouth.[40] Some commonly used instruments include sickle scalers which are designed with a pointed tip and are mainly used supragingivally.[39][40] Curettes are mainly used to remove subgingival calculus, smooth root surfaces and to clean out periodontal pockets.[39][43] Curettes can be divided into two subgroups: universals and area specific instruments. Universal curettes can be used in multiple areas, while area specific instruments are designed for select tooth surfaces.[40] Gracey curettes are a popular type of area specific curettes.[40] Due to their design, area specific curettes allow for better adaptation to the root surface and can be slightly more effective than universals.[39][40] Hoes, chisels, and files are less widely used than scalers and curettes. These are beneficial when removing large amounts of calculus or tenacious calculus that cannot be removed with a curette or scaler alone.[39] Chisels and hoes are used to remove bands of calculus, whereas files are used to crush burnished or tenacious calculus.[39]
Ultrasonic scalers, also known as power scalers, are effective in removing calculus, stain, and plaque. These scalers are also useful for root planing, curettage, and surgical debridement.[39] Not only is tenacious calculus and stain removed more effectively with ultrasonic scalers than with hand instrumentation alone, it is evident that the most satisfactory clinical results are when ultrasonics are used in adjunct to hand instrumentation.[39] There are two types of ultrasonic scalers; piezoelectric and magnetostrictive. Oscillating material in both of these handpieces cause the tip of the scaler to vibrate at high speeds, between 18,000 and 50,000Hz.[39] The tip of each scaler uses a different vibration pattern for removal of calculus.[39] The magnetostrictive power scaler vibration is elliptical, activating all sides of the tip, whereas the piezoelectric vibration is linear and is more active on the two sides of the tip.[39]
Special tips for ultrasonic scalers are designed to address different areas of the mouth and varying amounts of calculus buildup. Larger tips are used for heavy subgingival or supragingival calculus deposits, whereas thinner tips are designed more for definitive subgingival debridement.[39] As the high frequency vibrations loosen calculus and plaque, heat is generated at the tip.[39] A water spray is directed towards the end of the tip to cool it as well as irrigate the gingiva during debridement.[39] Only the first 1–2mm of the tip on the ultrasonic scaler is most effective for removal, and therefore needs to come into direct contact with the calculus to fracture the deposits.[39] Small adaptations are needed in order to keep the tip of the scaler touching the surface of the tooth, while overlapping oblique, horizontal, or vertical strokes are used for adequate calculus removal.[39]
Current research on potentially more effective methods of subgingival calculus removal focuses on the use of near-ultraviolet and near-infrared lasers, such as Er,Cr:YSGG lasers.[44][45] The use of lasers in periodontal therapy offers a unique clinical advantage over conventional hand instrumentation, as the thin and flexible fibers can deliver laser energy into periodontal pockets that are otherwise difficult to access.[45] Near-infrared lasers, such as the Er,CR:YSGG laser, have been proposed as an effective adjunct for calculus removal as the emission wavelength is highly absorbed by water, a large component of calculus deposits.[45] An optimal output power setting of 1.0-W with the near-infrared Er,Cr:YSGG laser has been shown to be effective for root scaling.[45] Near-ultraviolet lasers have also shown promise as they allow the dental professional to remove calculus deposits quickly, without removing underlying healthy tooth structure, which often occurs during hand instrumentation.[44] Additionally, near-ultraviolet lasers are effective at various irradiation angles for calculus removal.[44] Discrepancies in the efficiency of removal are due to the physical and optical properties of the calculus deposits, not to the angle of laser use.[44] Dental hygienists must receive additional theoretical and clinical training on the use of lasers, where legislation permits.[46]
Periodontal disease, also known as gum disease, is a set of inflammatory conditions affecting the tissues surrounding the teeth. In its early stage, called gingivitis, the gums become swollen and red and may bleed. It is considered the main cause of tooth loss for adults worldwide. In its more serious form, called periodontitis, the gums can pull away from the tooth, bone can be lost, and the teeth may loosen or fall out. Halitosis may also occur.
Periodontology or periodontics is the specialty of dentistry that studies supporting structures of teeth, as well as diseases and conditions that affect them. The supporting tissues are known as the periodontium, which includes the gingiva (gums), alveolar bone, cementum, and the periodontal ligament. A periodontist is a dentist that specializes in the prevention, diagnosis and treatment of periodontal disease and in the placement of dental implants.
Dental plaque is a biofilm of microorganisms that grows on surfaces within the mouth. It is a sticky colorless deposit at first, but when it forms tartar, it is often brown or pale yellow. It is commonly found between the teeth, on the front of teeth, behind teeth, on chewing surfaces, along the gumline (supragingival), or below the gumline cervical margins (subgingival). Dental plaque is also known as microbial plaque, oral biofilm, dental biofilm, dental plaque biofilm or bacterial plaque biofilm. Bacterial plaque is one of the major causes for dental decay and gum disease.
The gingival sulcus is an area of potential space between a tooth and the surrounding gingival tissue and is lined by sulcular epithelium. The depth of the sulcus is bounded by two entities: apically by the gingival fibers of the connective tissue attachment and coronally by the free gingival margin. A healthy sulcular depth is three millimeters or less, which is readily self-cleansable with a properly used toothbrush or the supplemental use of other oral hygiene aids.
Bleeding on probing (BoP) which is also known as bleeding gums or gingival bleeding is a term used by dentists and dental hygienists when referring to bleeding that is induced by gentle manipulation of the tissue at the depth of the gingival sulcus, or interface between the gingiva and a tooth. BoP is a sign of periodontal inflammation and indicates some sort of destruction and erosion to the lining of the sulcus or the ulceration of sulcular epithelium. The blood comes from lamina propria after the ulceration of the lining. BoP seems to be correlated with Periodontal Inflamed Surface Area (PISA).
Scaling and root planing, also known as conventional periodontal therapy, non-surgical periodontal therapy or deep cleaning, is a procedure involving removal of dental plaque and calculus and then smoothing, or planing, of the (exposed) surfaces of the roots, removing cementum or dentine that is impregnated with calculus, toxins, or microorganisms, the agents that cause inflammation. It is a part of non-surgical periodontal therapy. This helps to establish a periodontium that is in remission of periodontal disease. Periodontal scalers and periodontal curettes are some of the tools involved.
Gingival enlargement is an increase in the size of the gingiva (gums). It is a common feature of gingival disease. Gingival enlargement can be caused by a number of factors, including inflammatory conditions and the side effects of certain medications. The treatment is based on the cause. A closely related term is epulis, denoting a localized tumor on the gingiva.
Gingivectomy is a dental procedure in which a dentist or oral surgeon cuts away part of the gums in the mouth.
The periodontal curette is a type of hand-activated instrument used in dentistry and dental hygiene for the purpose of scaling and root planing. The periodontal curette is considered a treatment instrument and is classified into two main categories: universal curettes and Gracey curettes. Periodontal curettes have one face, one or two cutting edges and a rounded back and rounded toe. They are typically the instrument of choice for subgingival calculus removal.
Periodontal scalers are dental instruments used in the prophylactic and periodontal care of teeth, including scaling and root planing. The working ends come in a variety of shapes and sizes, but they are always narrow at the tip, so as to allow for access to narrow embrasure spaces between teeth. They differ from periodontal curettes, which possess a blunt tip.
Oral hygiene is the practice of keeping one's oral cavity clean and free of disease and other problems by regular brushing of the teeth and adopting good hygiene habits. It is important that oral hygiene be carried out on a regular basis to enable prevention of dental disease and bad breath. The most common types of dental disease are tooth decay and gum diseases, including gingivitis, and periodontitis.
Laser-assisted new attachment procedure (LANAP) is a surgical therapy for the treatment of periodontitis, intended to work through regeneration rather than resection. This therapy and the laser used to perform it have been in use since 1994. It was developed by Robert H. Gregg II and Delwin McCarthy.
Gingivitis is a non-destructive disease that causes inflammation of the gums; ulitis is an alternative term. The most common form of gingivitis, and the most common form of periodontal disease overall, is in response to bacterial biofilms that are attached to tooth surfaces, termed plaque-induced gingivitis. Most forms of gingivitis are plaque-induced.
Gingival disease is a term used to group the diseases that affect the gingiva(gums). The most common gingival disease is gingivitis, the earliest stage of gingival-related diseases. Gingival disease encompasses all the conditions that surround the gums, this includes plaque-induced gingivitis, non-dental biofilm plaque-induced gingivitis, and periodontal diseases.
In dentistry, debridement refers to the removal by dental cleaning of accumulations of plaque and calculus (tartar) in order to maintain dental health. Debridement may be performed using ultrasonic instruments, which fracture the calculus, thereby facilitating its removal, as well as hand tools, including periodontal scaler and curettes, or through the use of chemicals such as hydrogen peroxide.
A periodontal abscess, is a localized collection of pus within the tissues of the periodontium. It is a type of dental abscess. A periodontal abscess occurs alongside a tooth, and is different from the more common periapical abscess, which represents the spread of infection from a dead tooth. To reflect this, sometimes the term "lateral (periodontal) abscess" is used. In contrast to a periapical abscess, periodontal abscesses are usually associated with a vital (living) tooth. Abscesses of the periodontium are acute bacterial infections classified primarily by location.
Chronic periodontitis is one of the seven categories of periodontitis as defined by the American Academy of Periodontology 1999 classification system. Chronic periodontitis is a common disease of the oral cavity consisting of chronic inflammation of the periodontal tissues that is caused by the accumulation of profuse amounts of dental plaque. Periodontitis initially begins as gingivitis and can progress onto chronic and subsequent aggressive periodontitis according to the 1999 classification.
Aggressive periodontitis describes a type of periodontal disease and includes two of the seven classifications of periodontitis as defined by the 1999 classification system:
Localized aggressive periodontitis (LAP)
Generalized aggressive periodontitis (GAP)
Periodontal surgery is a form of dental surgery that prevents or corrects anatomical, traumatic, developmental, or plaque-induced defects in the bone, gingiva, or alveolar mucosa. The objectives of this surgery include accessibility of instruments to root surface, elimination of inflammation, creation of an oral environment for plaque control, periodontal diseases control, oral hygiene maintenance, maintain proper embrasure space, address gingiva-alveolar mucosa problems, and esthetic improvement. The surgical procedures include crown lengthening, frenectomy, and mucogingival flap surgery.
↑ Hardy K, Blakeney T, Copeland L, Kirkham J, Wrangham R, Collins M (2009). "Starch granules, dental calculus and new perspectives on ancient diet". Journal of Archaeological Science. 36 (2): 248–255. Bibcode:2009JArSc..36..248H. doi:10.1016/j.jas.2008.09.015.
↑ Blatt SH, Redmond BG, Cassman V, Sciulli PW (2011). "Dirty teeth and ancient trade: evidence of cotton fibres in human dental calculus from Late Woodland, Ohio". International Journal of Osteoarchaeology. 21 (6): 669–678. doi:10.1002/oa.1173.
↑ A. Molokhia and G. S. Nixon, "Studies on the composition of human dental calculus. Determination of some major and trace elements by instrumental neutron activation analysis", Journal of Radioanalytical and Nuclear Chemistry, Volume 83, Number 2, August, 1984, p. 273-281. (abstract)
↑ Clayton YM, Fox EC (May 1973). "Investigations into the mycology of dental calculus in town-dwellers, agricultural workers and grazing animals". Journal of Periodontology. 44 (5): 281–5. doi:10.1902/jop.1973.44.5.281. PMID4572515.
↑ White DJ (October 1997). "Dental calculus: recent insights into occurrence, formation, prevention, removal and oral health effects of supragingival and subgingival deposits". European Journal of Oral Sciences. 105 (5 Pt 2): 508–22. doi:10.1111/j.1600-0722.1997.tb00238.x. PMID9395117.
↑ Nakano K, Nemoto H, Nomura R, Inaba H, Yoshioka H, Taniguchi K, Amano A, Ooshima T (February 2009). "Detection of oral bacteria in cardiovascular specimens". Oral Microbiology and Immunology. 24 (1): 64–8. doi:10.1111/j.1399-302x.2008.00479.x. PMID19121072.
↑ Yeo BK, Lim LP, Paquette DW, Williams RC (January 2005). "Periodontal disease -- the emergence of a risk for systemic conditions: pre-term low birth weight". Annals of the Academy of Medicine, Singapore. 34 (1): 111–6. doi:10.47102/annals-acadmedsg.V34N1p111. PMID15726229.
↑ "Parameter on systemic conditions affected by periodontal diseases. American Academy of Periodontology". Journal of Periodontology. 71 (5 Suppl): 880–3. May 2000. doi:10.1902/jop.2000.71.5-S.880. PMID10875699.
↑ Addy M, Richards J, Williams G (August 1980). "Effects of a zinc citrate mouthwash on dental plaque and salivary bacteria". Journal of Clinical Periodontology. 7 (4): 309–15. doi:10.1111/j.1600-051x.1980.tb01973.x. PMID7007451.
↑ Diekwisch TG (September 2001). "The developmental biology of cementum". The International Journal of Developmental Biology. 45 (5–6): 695–706. PMID11669371.
↑ Metcalf JL, Ursell LK, Knight R (April 2014). "Ancient human oral plaque preserves a wealth of biological data". Nature Genetics. 46 (4): 321–3. doi:10.1038/ng.2930. PMID24675519. S2CID27141424.
1 2 3 4 Ting CC, Fukuda M, Watanabe T, Aoki T, Sanaoka A, Noguchi T (November 2007). "Effects of Er,Cr:YSGG laser irradiation on the root surface: morphologic analysis and efficiency of calculus removal". Journal of Periodontology. 78 (11): 2156–64. doi:10.1902/jop.2007.070160. PMID17970683.
This page is based on this Wikipedia article Text is available under the CC BY-SA 4.0 license; additional terms may apply. Images, videos and audio are available under their respective licenses.