Alien hand syndrome (AHS) or Dr. Strangelove syndrome is a category of conditions in which a person experiences their limbs acting seemingly on their own, without conscious control over the actions. There are a variety of clinical conditions that fall under this category, which most commonly affects the left hand. There are many similar terms for the various forms of the condition, but they are often used inappropriately. The affected person may sometimes reach for objects and manipulate them without wanting to do so, even to the point of having to use the controllable hand to restrain the alien hand. Under normal circumstances however, given that intent and action can be assumed to be deeply mutually entangled, the occurrence of alien hand syndrome can be usefully conceptualized as a phenomenon reflecting a functional "disentanglement" between thought and action.

The frontal lobe is the largest of the four major lobes of the brain in mammals, and is located at the front of each cerebral hemisphere. It is parted from the parietal lobe by a groove between tissues called the central sulcus and from the temporal lobe by a deeper groove called the lateral sulcus. The most anterior rounded part of the frontal lobe is known as the frontal pole, one of the three poles of the cerebrum.

Frontotemporal dementia (FTD), also called frontotemporal degeneration disease or frontotemporal neurocognitive disorder, encompasses several types of dementia involving the progressive degeneration of the brain's frontal and temporal lobes. FTD is the second most prevalent type of early onset dementia after Alzheimer's disease. Men and women appear to be equally affected. FTD generally presents as a behavioral or language disorder with gradual onset. Signs and symptoms tend to appear in late adulthood, typically between the ages of 45 and 65, although it can affect people younger or older than this. Currently, no cure or approved symptomatic treatment for FTD exists, although some off-label drugs and behavioral methods are prescribed.
Amotivational syndrome is a chronic psychiatric disorder characterized by signs that are linked to cognitive and emotional states such as detachment, blunted emotion and drives, executive functions like memory and attention, disinterest, passivity, apathy, and a general lack of motivation. This syndrome can be branched into two subtypes - marijuana amotivational syndrome, interchangeably known as cannabis induced amotivational syndrome which is caused by usage and/or dependency of the substance and is primarily associated with long-term effects of cannabis use, and SSRI-induced amotivational syndrome or SSRI-induced apathy caused by the intake of SSRI medication dosage. According to the Handbook of Clinical Psychopharmacology for Therapists, amotivational syndrome is listed as a possible side effect of SSRIs in the treatment of clinical depression.
Frontal lobe epilepsy (FLE) is a neurological disorder that is characterized by brief, recurring seizures arising in the frontal lobes of the brain, that often occur during sleep. It is the second most common type of epilepsy after temporal lobe epilepsy (TLE), and is related to the temporal form in that both forms are characterized by partial (focal) seizures.
In cognitive science and neuropsychology, executive functions are a set of cognitive processes that are necessary for the cognitive control of behavior: selecting and successfully monitoring behaviors that facilitate the attainment of chosen goals. Executive functions include basic cognitive processes such as attentional control, cognitive inhibition, inhibitory control, working memory, and cognitive flexibility. Higher-order executive functions require the simultaneous use of multiple basic executive functions and include planning and fluid intelligence.
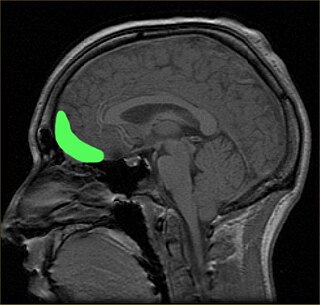
The orbitofrontal cortex (OFC) is a prefrontal cortex region in the frontal lobes of the brain which is involved in the cognitive process of decision-making. In non-human primates it consists of the association cortex areas Brodmann area 11, 12 and 13; in humans it consists of Brodmann area 10, 11 and 47.

Frontal lobe disorder, also frontal lobe syndrome, is an impairment of the frontal lobe of the brain due to disease or frontal lobe injury. The frontal lobe plays a key role in executive functions such as motivation, planning, social behaviour, and speech production. Frontal lobe syndrome can be caused by a range of conditions including head trauma, tumours, neurodegenerative diseases, neurodevelopmental disorders, neurosurgery and cerebrovascular disease. Frontal lobe impairment can be detected by recognition of typical signs and symptoms, use of simple screening tests, and specialist neurological testing.
Utilization behavior (UB) is a type of neurobehavioral phenomena that involves someone grabbing objects in view and starting the 'appropriate' behavior associated with it at an 'inappropriate' time. Patients exhibiting utilization behavior have difficulty resisting the impulse to operate or manipulate objects which are in their visual field and within reach. Characteristics of UB include unintentional, unconscious actions triggered by the immediate environment. The unpreventable excessive behavior has been linked to lesions in the frontal lobe. UB has also been referred to as "bilateral magnetic apraxia" and "hypermetamorphosis".
Perseveration, in the fields of psychology, psychiatry, and speech–language pathology, is the repetition of a particular response regardless of the absence or cessation of a stimulus. It is usually caused by a brain injury or other organic disorder. Symptoms include "lacking ability to transition or switch ideas appropriately with the social context, as evidenced by the repetition of words or gestures after they have ceased to be socially relevant or appropriate", or the "act or task of doing so", and are not better described as stereotypy.
Frontostriatal circuits are neural pathways that connect frontal lobe regions with the striatum and mediate motor, cognitive, and behavioural functions within the brain. They receive inputs from dopaminergic, serotonergic, noradrenergic, and cholinergic cell groups that modulate information processing. Frontostriatal circuits are part of the executive functions. Executive functions include the following: selection and perception of important information, manipulation of information in working memory, planning and organization, behavioral control, adaptation to changes, and decision making. These circuits are involved in neurodegenerative disorders such as Alzheimer's disease and Parkinson's disease as well as neuropsychiatric disorders including schizophrenia, depression, obsessive compulsive disorder (OCD), and in neurodevelopmental disorder such as attention-deficit hyperactivity disorder (ADHD).
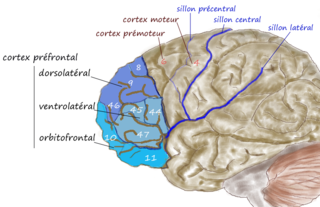
The dorsolateral prefrontal cortex is an area in the prefrontal cortex of the primate brain. It is one of the most recently derived parts of the human brain. It undergoes a prolonged period of maturation which lasts into adulthood. The DLPFC is not an anatomical structure, but rather a functional one. It lies in the middle frontal gyrus of humans. In macaque monkeys, it is around the principal sulcus. Other sources consider that DLPFC is attributed anatomically to BA 9 and 46 and BA 8, 9 and 10.
In psychology, impulsivity is a tendency to act on a whim, displaying behavior characterized by little or no forethought, reflection, or consideration of the consequences. Impulsive actions are typically "poorly conceived, prematurely expressed, unduly risky, or inappropriate to the situation that often result in undesirable consequences," which imperil long-term goals and strategies for success. Impulsivity can be classified as a multifactorial construct. A functional variety of impulsivity has also been suggested, which involves action without much forethought in appropriate situations that can and does result in desirable consequences. "When such actions have positive outcomes, they tend not to be seen as signs of impulsivity, but as indicators of boldness, quickness, spontaneity, courageousness, or unconventionality." Thus, the construct of impulsivity includes at least two independent components: first, acting without an appropriate amount of deliberation, which may or may not be functional; and second, choosing short-term gains over long-term ones.
The frontal lobe of the human brain is both relatively large in mass and less restricted in movement than the posterior portion of the brain. It is a component of the cerebral system, which supports goal directed behavior. This lobe is often cited as the part of the brain responsible for the ability to decide between good and bad choices, as well as recognize the consequences of different actions. Because of its location in the anterior part of the head, the frontal lobe is arguably more susceptible to injuries. Following a frontal lobe injury, an individual's abilities to make good choices and recognize consequences are often impaired. Memory impairment is another common effect associated with frontal lobe injuries, but this effect is less documented and may or may not be the result of flawed testing. Damage to the frontal lobe can cause increased irritability, which may include a change in mood and an inability to regulate behavior. Particularly, an injury of the frontal lobe could lead to deficits in executive function, such as anticipation, goal selection, planning, initiation, sequencing, monitoring, and self-correction. A widely reported case of frontal lobe injury was that of Phineas Gage, a railroad worker whose left frontal lobe was damaged by a large iron rod in 1848.
In psychology and neuroscience, executive dysfunction, or executive function deficit, is a disruption to the efficacy of the executive functions, which is a group of cognitive processes that regulate, control, and manage other cognitive processes. Executive dysfunction can refer to both neurocognitive deficits and behavioural symptoms. It is implicated in numerous psychopathologies and mental disorders, as well as short-term and long-term changes in non-clinical executive control. Executive dysfunction is the mechanism underlying ADHD Paralysis, and in a broader context, it can encompass other cognitive difficulties like planning, organizing, initiating tasks and regulating emotions. It is a core characteristic of ADHD and can elucidate numerous other recognized symptoms.
Kindling due to substance withdrawal is the neurological condition which results from repeated withdrawal episodes from sedative–hypnotic drugs such as alcohol and benzodiazepines.
Cerebellar cognitive affective syndrome (CCAS), also called Schmahmann's syndrome is a condition that follows from lesions (damage) to the cerebellum of the brain. It refers to a constellation of deficits in the cognitive domains of executive function, spatial cognition, language, and affect resulting from damage to the cerebellum. Impairments of executive function include problems with planning, set-shifting, abstract reasoning, verbal fluency, and working memory, and there is often perseveration, distractibility and inattention. Language problems include dysprosodia, agrammatism and mild anomia. Deficits in spatial cognition produce visual–spatial disorganization and impaired visual–spatial memory. Personality changes manifest as blunting of affect or disinhibited and inappropriate behavior. These cognitive impairments result in an overall lowering of intellectual function. CCAS challenges the traditional view of the cerebellum being responsible solely for regulation of motor functions. It is now thought that the cerebellum is responsible for monitoring both motor and nonmotor functions. The nonmotor deficits described in CCAS are believed to be caused by dysfunction in cerebellar connections to the cerebral cortex and limbic system.
Executive functions are a cognitive apparatus that controls and manages cognitive processes. Norman and Shallice (1980) proposed a model on executive functioning of attentional control that specifies how thought and action schemata become activated or suppressed for routine and non-routine circumstances. Schemas, or scripts, specify an individual's series of actions or thoughts under the influence of environmental conditions. Every stimulus condition turns on the activation of a response or schema. The initiation of appropriate schema under routine, well-learned situations is monitored by contention scheduling which laterally inhibits competing schemas for the control of cognitive apparatus. Under unique, non-routine procedures controls schema activation. The SAS is an executive monitoring system that oversees and controls contention scheduling by influencing schema activation probabilities and allowing for general strategies to be applied to novel problems or situations during automatic attentional processes.
Alcohol-related brain damage alters both the structure and function of the brain as a result of the direct neurotoxic effects of alcohol intoxication or acute alcohol withdrawal. Increased alcohol intake is associated with damage to brain regions including the frontal lobe, limbic system, and cerebellum, with widespread cerebral atrophy, or brain shrinkage caused by neuron degeneration. This damage can be seen on neuroimaging scans.
Organic personality disorder (OPD) or secondary personality change, is a condition described in the ICD-10 and ICD-11 respectively. It is characterized by a significant personality change featuring abnormal behavior due to an underlying traumatic brain injury or another pathophysiological medical condition affecting the brain. Abnormal behavior can include but is not limited to apathy, paranoia and disinhibition.