Related Research Articles
Under U.S. law, a conservatorship results from the appointment of a guardian or a protector by a judge to manage the personal or financial affairs of another person who is incapable of fully managing their own affairs due to age or physical or mental limitations. A person under conservatorship is a "conservatee", a term that can refer to an adult. A person under guardianship is a "ward", a term that can also refer to a minor child. Conservatorship may also apply to corporations and organizations.

Informed consent is a principle in medical ethics and medical law and media studies, that a patient must have sufficient information and understanding before making decisions about their medical care. Pertinent information may include risks and benefits of treatments, alternative treatments, the patient's role in treatment, and their right to refuse treatment. In most systems, healthcare providers have a legal and ethical responsibility to ensure that a patient's consent is informed. This principle applies more broadly than healthcare intervention, for example to conduct research and to disclose a person's medical information.

A power of attorney (POA) or letter of attorney is a written authorization to represent or act on another's behalf in private affairs, business, or some other legal matter. The person authorizing the other to act is the principal, grantor, or donor. The one authorized to act is the agent, attorney, or in some common law jurisdictions, the attorney-in-fact.

An advance healthcare directive, also known as living will, personal directive, advance directive, medical directive or advance decision, is a legal document in which a person specifies what actions should be taken for their health if they are no longer able to make decisions for themselves because of illness or incapacity. In the U.S. it has a legal status in itself, whereas in some countries it is legally persuasive without being a legal document.
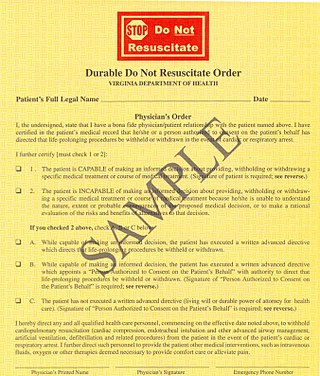
A do-not-resuscitate order (DNR), also known as Do Not Attempt Resuscitation (DNAR), Do Not Attempt Cardiopulmonary Resuscitation (DNACPR), no code or allow natural death, is a medical order, written or oral depending on the jurisdiction, indicating that a person should not receive cardiopulmonary resuscitation (CPR) if that person's heart stops beating. Sometimes these decisions and the relevant documents also encompass decisions around other critical or life-prolonging medical interventions. The legal status and processes surrounding DNR orders vary in different polities. Most commonly, the order is placed by a physician based on a combination of medical judgement and patient involvement.
In developmental psychology and moral, political, and bioethical philosophy, autonomy is the capacity to make an informed, uncoerced decision. Autonomous organizations or institutions are independent or self-governing. Autonomy can also be defined from a human resources perspective, where it denotes a level of discretion granted to an employee in his or her work. In such cases, autonomy is known to generally increase job satisfaction. Self-actualized individuals are thought to operate autonomously of external expectations. In a medical context, respect for a patient's personal autonomy is considered one of many fundamental ethical principles in medicine.
Medical ethics is an applied branch of ethics which analyzes the practice of clinical medicine and related scientific research. Medical ethics is based on a set of values that professionals can refer to in the case of any confusion or conflict. These values include the respect for autonomy, non-maleficence, beneficence, and justice. Such tenets may allow doctors, care providers, and families to create a treatment plan and work towards the same common goal. It is important to note that these four values are not ranked in order of importance or relevance and that they all encompass values pertaining to medical ethics. However, a conflict may arise leading to the need for hierarchy in an ethical system, such that some moral elements overrule others with the purpose of applying the best moral judgement to a difficult medical situation. Medical ethics is particularly relevant in decisions regarding involuntary treatment and involuntary commitment.
The Uniform Rights of the Terminally Ill Act, was recommended as a Uniform Act in the United States. The Uniform Rights of the Terminally Ill Act subsequently was passed by many states. The Uniform Rights of the Terminally Ill Act was replaced as a recommended Uniform act by the Uniform Health-Care Decision-making Act in 1993. The law allows a person to declare a living will specifying that, if the situation arises, he or she does not wish to be kept alive through life support if terminally ill or in a coma. The patient may also obtain a health care power of attorney. This power of attorney appoints an agent to make medical decision for the patient in case the patient becomes incompetent.
The right to die is a concept based on the opinion that human beings are entitled to end their life or undergo voluntary euthanasia. Possession of this right is often understood that a person with a terminal illness, incurable pain, or without the will to continue living, should be allowed to end their own life, use assisted suicide, or to decline life-prolonging treatment. The question of who, if anyone, may be empowered to make this decision is often the subject of debate.
Estate planning is the process of anticipating and arranging for the management and disposal of a person's estate during the person's life in preparation for a person's future incapacity or death. The planning includes the bequest of assets to heirs, loved ones, and/or charity, and may include minimizing gift, estate, and generation-skipping transfer taxes. Estate planning includes planning for incapacity, reducing or eliminating uncertainties over the administration of a probate, and maximizing the value of the estate by reducing taxes and other expenses. The ultimate goal of estate planning can only be determined by the specific goals of the estate owner, and may be as simple or complex as the owner's wishes and needs directs. Guardians are often designated for minor children and beneficiaries with incapacity.
A legal guardian is a person who has been appointed by a court or otherwise has the legal authority to make decisions relevant to the personal and property interests of another person who is deemed incompetent, called a ward. For example, a legal guardian might be granted the authority to make decisions regarding a ward's housing or medical care or manage the ward's finances. Guardianship is most appropriate when an alleged ward is functionally incapacitated, meaning they have a lagging skill critical to performing certain tasks, such as making important life decisions. Guardianship intends to serve as a safeguard to protect the ward.
A person's next of kin (NOK) may be that person's spouse, adopted family member or closest living blood relative. Some countries, such as the United States, have a legal definition of "next of kin". In other countries, such as the United Kingdom, "next of kin" may have no legal definition and may not necessarily refer to blood relatives at all.
In United States and Canadian law, competence concerns the mental capacity of an individual to participate in legal proceedings or transactions, and the mental condition a person must have to be responsible for his or her decisions or acts. Competence is an attribute that is decision-specific. Depending on various factors which typically revolve around mental function integrity, an individual may or may not be competent to make a particular medical decision, a particular contractual agreement, to execute an effective deed to real property, or to execute a will having certain terms.
Elder law denotes the law, regulations, and prevailing good legal practices applicable to a range of issues affecting individuals aged 65 and over.
Five Wishes is a United States advance directive created by the non-profit organization Aging with Dignity. It has been described as the "living will with a heart and soul".
The Family Health Care Decisions Act is a statute adopted in New York state in 2010 that had been pending before the legislature since 1994. The statute was approved by the New York State Senate in July, 2009. The legislation was introduced by state senator Thomas Duane of Manhattan. It was signed into law by Gov. David Paterson on March 16, 2010.
A surrogate decision maker, also known as a health care proxy or as agents, is an advocate for incompetent patients. If a patient is unable to make decisions for themselves about personal care, some agent must make decisions for them. If there is a durable power of attorney for health care, the agent appointed by that document is authorized to make health care decisions within the scope of authority granted by the document. If people have court-appointed guardians with authority to make health care decisions, the guardian is the authorized surrogate.
Advance care planning is a process that enables individuals to make plans about their future health care. Advance care plans provide direction to healthcare professionals when a person is not in a position to make and/or communicate their own healthcare choices. Advance care planning is applicable to adults at all stages of life. Participation in advance care planning has been shown to reduce stress and anxiety for patients and their families, and lead to improvements in end of life care. Older adults are more directly concerned as they may experience a situation where advance care planning can be useful. However, a minority use them. A research conducted in Switzerland with people aged 71 to 80 showed that better knowledge on advance care planning dispositions could improve the perception older people have of them. Communication on dispositions should take into account individual knowledge levels and address commonly enunciated barriers that seem to diminish with increased knowledge.
Act 39 of 2013 established the U.S. state of Vermont's Patient Choice and Control at End of Life Act, which legalizes medical aid in dying with certain restrictions. Vermont was the first state to enact this Law through legislative action; it permits some terminally ill patients to determine the time of their own death.
In the law of England and Wales, best interest decisions are decisions made on behalf of people who do not have mental capacity to make them for themselves at the time the decision needs to be taken. Someone who has the capacity to make a decision is said to be "capacitous". Since 2007, there has been a dedicated court with jurisdiction over mental capacity: the Court of Protection, although it mostly deals with adults. Most applications to make decisions on behalf of a child are still dealt with by the Family Court.
References
- 1 2 "Health Care Proxy - New York State Department of Health" (PDF). New York State Department of Health. Archived from the original (PDF) on 2014-06-11.
- ↑ "General Law - Part II, Title II, Chapter 201D, Section 4". malegislature.gov. Retrieved 2018-10-30.
- ↑ "Healthcare Proxy - Who Will Speak for You?". www.health.ny.gov. Retrieved 2018-10-29.
- 1 2 Moye J, Sabatino CP, Weintraub Brendel R (April 2013). "Evaluation of the capacity to appoint a healthcare proxy". The American Journal of Geriatric Psychiatry. 21 (4): 326–36. doi:10.1016/j.jagp.2012.09.001. PMC 4859336 . PMID 23498379.
- ↑ "Health Care Proxy/Living Will | Stony Brook Medicine". www.stonybrookmedicine.edu. Retrieved 2018-10-29.
- ↑ Sabatino CP (June 2010). "The evolution of healthcare advance planning law and policy". The Milbank Quarterly. 88 (2): 211–39. doi:10.1111/j.1468-0009.2010.00596.x. PMC 2980344 . PMID 20579283.
- 1 2 3 Rai A (September 1999). "The Physician as a Healthcare Proxy". The Hastings Center Report. Hastings Center. Retrieved 2007-10-14.
- ↑ Hack J, Buecking B, Lopez CL, Ruchholtz S, Kühne CA (December 2016). "[Living will, durable power of attorney and legal guardianship in the trauma surgery routine : Data from a geriatric trauma center]". Zeitschrift für Gerontologie und Geriatrie (in German). 49 (8): 721–726. doi:10.1007/s00391-015-0981-1. PMID 26608036. S2CID 32809957.
- ↑ Health Care Powers of Attorney: Interactive Map, LawServer. Retrieved on August 19, 2014.
- ↑ Meier, Diane E.; Isaacs, Stephen L.; Hughes, Robert, eds. (2011). Palliative Care: Transforming the Care of Serious Illness. Germany: Wiley. p. 170. ISBN 978-1-118-03964-9.
- ↑ "Myths and Facts About Health Care Advance Directives" (PDF). ABA Commission on Law and Aging. American Bar Association. Retrieved 8 May 2017.