
Acute disseminated encephalomyelitis (ADEM), or acute demyelinating encephalomyelitis, is a rare autoimmune disease marked by a sudden, widespread attack of inflammation in the brain and spinal cord. As well as causing the brain and spinal cord to become inflamed, ADEM also attacks the nerves of the central nervous system and damages their myelin insulation, which, as a result, destroys the white matter. The cause is often a trigger such as from viral infection or vaccinations.

Central pontine myelinolysis is a neurological condition involving severe damage to the myelin sheath of nerve cells in the pons. It is predominately iatrogenic (treatment-induced), and is characterized by acute paralysis, dysphagia, dysarthria, and other neurological symptoms.

White matter refers to areas of the central nervous system (CNS) that are mainly made up of myelinated axons, also called tracts. Long thought to be passive tissue, white matter affects learning and brain functions, modulating the distribution of action potentials, acting as a relay and coordinating communication between different brain regions.
Vascular dementia (VaD) is dementia caused by problems in the blood supply to the brain, resulting from a cerebrovascular disease. Restricted blood supply (ischemia) leads to cell and tissue death in the affected region, known as an infarct. The three types of vascular dementia are subcortical vascular dementia, multi-infarct dementia, and stroke related dementia. Subcortical vascular dementia is brought about by damage to the small blood vessels in the brain. Multi-infarct dementia is brought about by a series of mini-strokes where many regions have been affected. The third type is stroke related where more serious damage may result. Such damage leads to varying levels of cognitive decline. When caused by mini-strokes the decline in cognition is gradual. When due to a stroke the cognitive decline can be traced back to the event.

Binswanger's disease, also known as subcortical leukoencephalopathy and subcortical arteriosclerotic encephalopathy, is a form of small-vessel vascular dementia caused by damage to the white brain matter. White matter atrophy can be caused by many circumstances including chronic hypertension as well as old age. This disease is characterized by loss of memory and intellectual function and by changes in mood. These changes encompass what are known as executive functions of the brain. It usually presents between 54 and 66 years of age, and the first symptoms are usually mental deterioration or stroke.

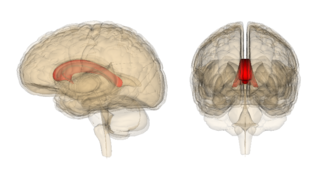
The caudate nucleus is one of the structures that make up the corpus striatum, which is a component of the basal ganglia in the human brain. While the caudate nucleus has long been associated with motor processes due to its role in Parkinson's disease, it plays important roles in various other nonmotor functions as well, including procedural learning, associative learning and inhibitory control of action, among other functions. The caudate is also one of the brain structures which compose the reward system and functions as part of the cortico–basal ganglia–thalamic loop.

Cognitive disorders (CDs), also known as neurocognitive disorders (NCDs), are a category of mental health disorders that primarily affect cognitive abilities including learning, memory, perception, and problem-solving. Neurocognitive disorders include delirium, mild neurocognitive disorders, and major neurocognitive disorder (previously known as dementia). They are defined by deficits in cognitive ability that are acquired (as opposed to developmental), typically represent decline, and may have an underlying brain pathology. The DSM-5 defines six key domains of cognitive function: executive function, learning and memory, perceptual-motor function, language, complex attention, and social cognition.
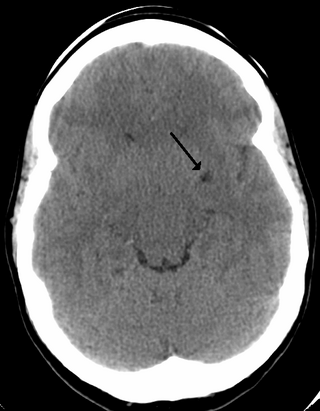
Cerebral atrophy is a common feature of many of the diseases that affect the brain. Atrophy of any tissue means a decrement in the size of the cell, which can be due to progressive loss of cytoplasmic proteins. In brain tissue, atrophy describes a loss of neurons and the connections between them. Brain atrophy can be classified into two main categories: generalized and focal atrophy. Generalized atrophy occurs across the entire brain whereas focal atrophy affects cells in a specific location. If the cerebral hemispheres are affected, conscious thought and voluntary processes may be impaired.
Semantic dementia (SD), also known as semantic variant primary progressive aphasia (svPPA), is a progressive neurodegenerative disorder characterized by loss of semantic memory in both the verbal and non-verbal domains. However, the most common presenting symptoms are in the verbal domain. Semantic dementia is a disorder of semantic memory that causes patients to lose the ability to match words or images to their meanings. However, it is fairly rare for patients with semantic dementia to develop category specific impairments, though there have been documented cases of it occurring. Typically, a more generalized semantic impairment results from dimmed semantic representations in the brain.
A perivascular space, also known as a Virchow–Robin space, is a fluid-filled space surrounding certain blood vessels in several organs, including the brain, potentially having an immunological function, but more broadly a dispersive role for neural and blood-derived messengers. The brain pia mater is reflected from the surface of the brain onto the surface of blood vessels in the subarachnoid space. In the brain, perivascular cuffs are regions of leukocyte aggregation in the perivascular spaces, usually found in patients with viral encephalitis.
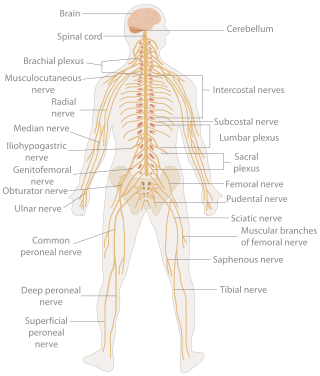
A neurological examination is the assessment of sensory neuron and motor responses, especially reflexes, to determine whether the nervous system is impaired. This typically includes a physical examination and a review of the patient's medical history, but not deeper investigation such as neuroimaging. It can be used both as a screening tool and as an investigative tool, the former of which when examining the patient when there is no expected neurological deficit and the latter of which when examining a patient where you do expect to find abnormalities. If a problem is found either in an investigative or screening process, then further tests can be carried out to focus on a particular aspect of the nervous system.
Pseudobulbar palsy is a medical condition characterized by the inability to control facial movements and caused by a variety of neurological disorders. Patients experience difficulty chewing and swallowing, have increased reflexes and spasticity in tongue and the bulbar region, and demonstrate slurred speech, sometimes also demonstrating uncontrolled emotional outbursts.
Marchiafava–Bignami disease is a progressive neurological disease of alcohol use disorder, characterized by corpus callosum demyelination and necrosis and subsequent atrophy. The disease was first described in 1903 by the Italian pathologists Amico Bignami and Ettore Marchiafava in an Italian Chianti drinker. In this autopsy, Marchiafava and Bignami noticed that the middle two-thirds of the corpus callosum were necrotic. It is very difficult to diagnose and there is no specific treatment. Until 2008 only around 300 cases had been reported. If caught early enough, most patients survive.
Mild cognitive impairment (MCI) is a neurocognitive disorder which involves cognitive impairments beyond those expected based on an individual's age and education but which are not significant enough to interfere with instrumental activities of daily living. MCI may occur as a transitional stage between normal aging and dementia, especially Alzheimer's disease. It includes both memory and non-memory impairments. The cause of the disorder remains unclear, as well as both its prevention and treatment, with some 50 percent of people diagnosed with it going on to develop Alzheimer's disease within five years. The diagnosis can also serve as an early indicator for other types of dementia, although MCI may remain stable or even remit.
Subcortical ischemic depression, also known as vascular depression, is a medical condition most commonly seen in older people with major depressive disorder. Subcortical ischemic depression refers to vascular depression specifically due to lesions and restricted blood flow, known as ischemia, in certain parts of the brain. However, the disorder is typically described as vascular depression in the literature.
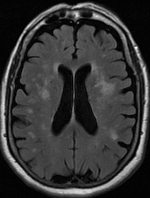
Leukoaraiosis is a particular abnormal change in appearance of white matter near the lateral ventricles. It is often seen in aged individuals, but sometimes in young adults. On MRI, leukoaraiosis changes appear as white matter hyperintensities (WMHs) in T2 FLAIR images. On CT scans, leukoaraiosis appears as hypodense periventricular white-matter lesions.
Alzheimer's Disease Neuroimaging Initiative (ADNI) is a multisite study that aims to improve clinical trials for the prevention and treatment of Alzheimer's disease (AD). This cooperative study combines expertise and funding from the private and public sector to study subjects with AD, as well as those who may develop AD and controls with no signs of cognitive impairment. Researchers at 63 sites in the US and Canada track the progression of AD in the human brain with neuroimaging, biochemical, and genetic biological markers. This knowledge helps to find better clinical trials for the prevention and treatment of AD. ADNI has made a global impact, firstly by developing a set of standardized protocols to allow the comparison of results from multiple centers, and secondly by its data-sharing policy which makes available all at the data without embargo to qualified researchers worldwide. To date, over 1000 scientific publications have used ADNI data. A number of other initiatives related to AD and other diseases have been designed and implemented using ADNI as a model. ADNI has been running since 2004 and is currently funded until 2021.

Harding ataxia is an autosomal recessive cerebellar ataxia originally described by Harding in 1981. This form of cerebellar ataxia is similar to Friedreich ataxia including that it results in poor reflexes and balance, but differs in several ways, including the absence of diabetes mellitus, optic atrophy, cardiomyopathy, skeletal abnormalities, and the fact that tendon reflexes in the arms and knees remain intact. This form of ataxia is characterized by onset in the first 20 years, and is less severe than Friedreich ataxia. Additional cases were diagnosed in 1989, 1990, 1991, and 1998.
Schizophrenia is a primary psychotic disorder, whereas, bipolar disorder is a primary mood disorder which can also involve psychosis. Both schizophrenia and bipolar disorder are characterized as critical psychiatric disorders in the Diagnostic and Statistical Manual of Mental Disorders fifth edition (DSM-5). However, because of some similar symptoms, differentiating between the two can sometimes be difficult; indeed, there is an intermediate diagnosis termed schizoaffective disorder.

neuGRID is a web portal aimed to (i) help neuroscientists do high-throughput imaging research, and (ii) provide clinical neurologists automated diagnostic imaging markers of neurodegenerative diseases for individual patient diagnosis. neuGRID's user-friendly environment is customised to a range of users from students to senior neuroscientists working in the fields of Alzheimer's disease, psychiatric diseases, and white matter diseases. neuGRID aims to become a widespread resource for brain imaging analyses.
