Related Research Articles

An advance healthcare directive, also known as living will, personal directive, advance directive, medical directive or advance decision, is a legal document in which a person specifies what actions should be taken for their health if they are no longer able to make decisions for themselves because of illness or incapacity. In the U.S. it has a legal status in itself, whereas in some countries it is legally persuasive without being a legal document.
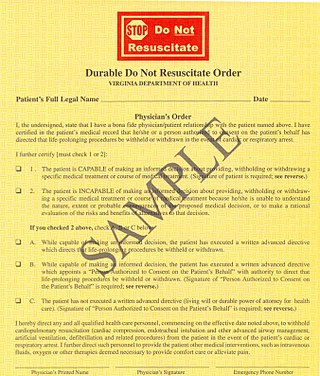
A do-not-resuscitate order (DNR), also known as Do Not Attempt Resuscitation (DNAR), Do Not Attempt Cardiopulmonary Resuscitation (DNACPR), no code or allow natural death, is a medical order, written or oral depending on the jurisdiction, indicating that a person should not receive cardiopulmonary resuscitation (CPR) if that person's heart stops beating. Sometimes these decisions and the relevant documents also encompass decisions around other critical or life-prolonging medical interventions. The legal status and processes surrounding DNR orders vary in different polities. Most commonly, the order is placed by a physician based on a combination of medical judgement and patient involvement.

Life support comprises the treatments and techniques performed in an emergency in order to support life after the failure of one or more vital organs. Healthcare providers and emergency medical technicians are generally certified to perform basic and advanced life support procedures; however, basic life support is sometimes provided at the scene of an emergency by family members or bystanders before emergency services arrive. In the case of cardiac injuries, cardiopulmonary resuscitation is initiated by bystanders or family members 25% of the time. Basic life support techniques, such as performing CPR on a victim of cardiac arrest, can double or even triple that patient's chance of survival. Other types of basic life support include relief from choking, staunching of bleeding by direct compression and elevation above the heart, first aid, and the use of an automated external defibrillator.
Palliative care is an interdisciplinary medical caregiving approach aimed at optimizing quality of life and mitigating suffering among people with serious, complex, and often terminal illnesses. Within the published literature, many definitions of palliative care exist. The World Health Organization (WHO) describes palliative care as "an approach that improves the quality of life of patients and their families facing the problems associated with life-threatening illness, through the prevention and relief of suffering by means of early identification and impeccable assessment and treatment of pain and other problems, physical, psychosocial, and spiritual". In the past, palliative care was a disease specific approach, but today the WHO takes a broader patient-centered approach that suggests that the principles of palliative care should be applied as early as possible to any chronic and ultimately fatal illness. This shift was important because if a disease-oriented approach is followed, the needs and preferences of the patient are not fully met and aspects of care, such as pain, quality of life, and social support, as well as spiritual and emotional needs, fail to be addressed. Rather, a patient-centered model prioritizes relief of suffering and tailors care to increase the quality of life for terminally ill patients.
In medicine, specifically in end-of-life care, palliative sedation is the palliative practice of relieving distress in a terminally ill person in the last hours or days of a dying person's life, usually by means of a continuous intravenous or subcutaneous infusion of a sedative drug, or by means of a specialized catheter designed to provide comfortable and discreet administration of ongoing medications via the rectal route.
Terminal illness or end-stage disease is a disease that cannot be cured or adequately treated and is expected to result in the death of the patient. This term is more commonly used for progressive diseases such as cancer, dementia or advanced heart disease than for injury. In popular use, it indicates a disease that will progress until death with near absolute certainty, regardless of treatment. A patient who has such an illness may be referred to as a terminal patient, terminally ill or simply as being terminal. There is no standardized life expectancy for a patient to be considered terminal, although it is generally months or less. Life expectancy for terminal patients is a rough estimate given by the physician based on previous data and does not always reflect true longevity. An illness which is lifelong but not fatal is a chronic condition.
Prognosis is a medical term for predicting the likelihood or expected development of a disease, including whether the signs and symptoms will improve or worsen or remain stable over time; expectations of quality of life, such as the ability to carry out daily activities; the potential for complications and associated health issues; and the likelihood of survival. A prognosis is made on the basis of the normal course of the diagnosed disease, the individual's physical and mental condition, the available treatments, and additional factors. A complete prognosis includes the expected duration, function, and description of the course of the disease, such as progressive decline, intermittent crisis, or sudden, unpredictable crisis.
Futile medical care is the continued provision of medical care or treatment to a patient when there is no reasonable hope of a cure or benefit.
Chronic care refers to medical care which addresses pre-existing or long-term illness, as opposed to acute care which is concerned with short term or severe illness of brief duration. Chronic medical conditions include asthma, diabetes, emphysema, chronic bronchitis, congestive heart disease, cirrhosis of the liver, hypertension and depression. Without effective treatment chronic conditions may lead to disability.
End-of-life care refers to health care provided in the time leading up to a person's death. End-of-life care can be provided in the hours, days, or months before a person dies and encompasses care and support for a person's mental and emotional needs, physical comfort, spiritual needs, and practical tasks.
The philosophy of healthcare is the study of the ethics, processes, and people which constitute the maintenance of health for human beings. For the most part, however, the philosophy of healthcare is best approached as an indelible component of human social structures. That is, the societal institution of healthcare can be seen as a necessary phenomenon of human civilization whereby an individual continually seeks to improve, mend, and alter the overall nature and quality of their life. This perennial concern is especially prominent in modern political liberalism, wherein health has been understood as the foundational good necessary for public life.

In the United States, hospice care is a type and philosophy of end-of-life care which focuses on the palliation of a terminally ill patient's symptoms. These symptoms can be physical, emotional, spiritual or social in nature. The concept of hospice as a place to treat the incurably ill has been evolving since the 11th century. Hospice care was introduced to the United States in the 1970s in response to the work of Cicely Saunders in the United Kingdom. This part of health care has expanded as people face a variety of issues with terminal illness. In the United States, it is distinguished by extensive use of volunteers and a greater emphasis on the patient's psychological needs in coming to terms with dying.
Hospice care is a type of health care that focuses on the palliation of a terminally ill patient's pain and symptoms and attending to their emotional and spiritual needs at the end of life. Hospice care prioritizes comfort and quality of life by reducing pain and suffering. Hospice care provides an alternative to therapies focused on life-prolonging measures that may be arduous, likely to cause more symptoms, or are not aligned with a person's goals.
In 2006, hospice and palliative medicine was officially recognized by the American Board of Medical Specialties, and is co-sponsored by the American Boards of
Pain in cancer may arise from a tumor compressing or infiltrating nearby body parts; from treatments and diagnostic procedures; or from skin, nerve and other changes caused by a hormone imbalance or immune response. Most chronic (long-lasting) pain is caused by the illness and most acute (short-term) pain is caused by treatment or diagnostic procedures. However, radiotherapy, surgery and chemotherapy may produce painful conditions that persist long after treatment has ended.
POLST is an approach to improving end-of-life care in the United States, encouraging providers to speak with the severely ill and create specific medical orders to be honored by health care workers during a medical crisis. POLST began in Oregon in 1991 and currently exists in 46 states; some of the 46 states have the program in development. The POLST document is a standardized, portable, brightly colored single page medical order that documents a conversation between a provider and an individual with a serious illness or frailty towards the end of life. A POLST form allows emergency medical services to provide treatment that the individual prefers before possibly transporting to an emergency facility.

Cultural competence in healthcare refers to the ability for healthcare professionals to demonstrate cultural competence toward patients with diverse values, beliefs, and feelings. This process includes consideration of the individual social, cultural, and psychological needs of patients for effective cross-cultural communication with their health care providers. The goal of cultural competence in health care is to reduce health disparities and to provide optimal care to patients regardless of their race, gender, ethnic background, native languages spoken, and religious or cultural beliefs. Cultural competency training is important in health care fields where human interaction is common, including medicine, nursing, allied health, mental health, social work, pharmacy, oral health, and public health fields.
Undertreatment of pain is the absence of pain management therapy for a person in pain when treatment is indicated.

End Game is a 2018 American short documentary film by Rob Epstein and Jeffrey Friedman about terminally ill patients in a San Francisco hospital meeting medical practitioners seeking to change the perception around life and death. The film was executive produced by Steven Ungerleider and Shoshana R. Ungerleider. It was released by Netflix.
The taxonomy of the burden of treatment is a visualization created for health care professionals to better comprehend the obstacles that interfere with a patient's health care plan. It was created as a result of a worldwide, qualitative-based study that asked adults with chronic conditions to list the personal, environmental, and financial barriers that burden a patient. The purpose of this visualization is to help health care providers develop personalized management strategies that the patient can follow through a narrative paradigm. The goal is to target interventions, achieve an interpersonal doctor-patient relationship, and improve health outcomes.
References
- 1 2 3 4 Gawande, Atul (2 August 2010). "Letting Go: What should medicine do when it can't save your life?". The New Yorker.
- ↑ Fister, Kristina (2007). "Short Cuts: What's New in the Other General Journals". BMJ: British Medical Journal. 334 (7590): 390–391. ISSN 0959-8138.
- ↑ Bogaty, Peter; Brophy, James M. (11 October 2006). "Acute ischemic heart disease and interventional cardiology: a time for pause". BMC Medicine. 4 (1): 25. doi:10.1186/1741-7015-4-25. ISSN 1741-7015.