
Abdominal pain, also known as a stomach ache, Is a symptom associated with both non-serious and serious medical issues. Since the abdomen contains most of the body's vital organs, it can be an indicator of a wide variety of diseases. Given that, approaching the examination of a person and planning of a differential diagnosis is extremely important.

The mesentery is an organ that attaches the intestines to the posterior abdominal wall and is formed by the double fold of peritoneum. It helps in storing fat and allowing blood vessels, lymphatics, and nerves to supply the intestines, among other functions.

A Meckel's diverticulum, a true congenital diverticulum, is a slight bulge in the small intestine present at birth and a vestigial remnant of the vitelline duct. It is the most common malformation of the gastrointestinal tract and is present in approximately 2% of the population, with males more frequently experiencing symptoms.

Omphalocele or omphalocoele also called exomphalos, is a rare abdominal wall defect. Beginning at the 6th week of development, rapid elongation of the gut and increased liver size reduces intra abdominal space, which pushes intestinal loops out of the abdominal cavity. Around 10th week, the intestine returns to the abdominal cavity and the process is completed by the 12th week. Persistence of intestine or the presence of other abdominal viscera in the umbilical cord results in an omphalocele.
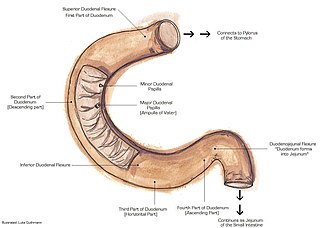
The suspensory muscle of duodenum is a thin muscle connecting the junction between the duodenum and jejunum, as well as the duodenojejunal flexure to connective tissue surrounding the superior mesenteric and coeliac arteries. The suspensory muscle most often connects to both the third and fourth parts of the duodenum, as well as the duodenojejunal flexure, although the attachment is quite variable.
Colic in horses is defined as abdominal pain, but it is a clinical symptom rather than a diagnosis. The term colic can encompass all forms of gastrointestinal conditions which cause pain as well as other causes of abdominal pain not involving the gastrointestinal tract. What makes it tricky is that different causes can manifest with similar signs of distress in the animal. Recognizing and understanding these signs is pivotal, as timely action can spell the difference between a brief moment of discomfort and a life-threatening situation. The most common forms of colic are gastrointestinal in nature and are most often related to colonic disturbance. There are a variety of different causes of colic, some of which can prove fatal without surgical intervention. Colic surgery is usually an expensive procedure as it is major abdominal surgery, often with intensive aftercare. Among domesticated horses, colic is the leading cause of premature death. The incidence of colic in the general horse population has been estimated between 4 and 10 percent over the course of the average lifespan. Clinical signs of colic generally require treatment by a veterinarian. The conditions that cause colic can become life-threatening in a short period of time.

A volvulus is when a loop of intestine twists around itself and the mesentery that supports it, resulting in a bowel obstruction. Symptoms include abdominal pain, abdominal bloating, vomiting, constipation, and bloody stool. Onset of symptoms may be rapid or more gradual. The mesentery may become so tightly twisted that blood flow to part of the intestine is cut off, resulting in ischemic bowel. In this situation there may be fever or significant pain when the abdomen is touched.

Gastrointestinal perforation, also known as gastrointestinal rupture, is a hole in the wall of the gastrointestinal tract. The gastrointestinal tract is composed of hollow digestive organs leading from the mouth to the anus. Symptoms of gastrointestinal perforation commonly include severe abdominal pain, nausea, and vomiting. Complications include a painful inflammation of the inner lining of the abdominal wall and sepsis.

Annular pancreas is a rare condition in which the second part of the duodenum is surrounded by a ring of pancreatic tissue continuous with the head of the pancreas. This portion of the pancreas can constrict the duodenum and block or impair the flow of food to the rest of the intestines. It is estimated to occur in 1 out of 12,000 to 15,000 newborns. The ambiguity arises from the fact that not all cases are symptomatic.

Ischemic colitis is a medical condition in which inflammation and injury of the large intestine result from inadequate blood supply. Although uncommon in the general population, ischemic colitis occurs with greater frequency in the elderly, and is the most common form of bowel ischemia. Causes of the reduced blood flow can include changes in the systemic circulation or local factors such as constriction of blood vessels or a blood clot. In most cases, no specific cause can be identified.

Intestinal atresia is any congenital malformation of the structure of the intestine that causes bowel obstruction. The malformation can be a narrowing (stenosis), absence or malrotation of a portion of the intestine. These defects can either occur in the small or large intestine.

A bowel resection or enterectomy is a surgical procedure in which a part of an intestine (bowel) is removed, from either the small intestine or large intestine. Often the word enterectomy is reserved for the sense of small bowel resection, in distinction from colectomy, which covers the sense of large bowel resection. Bowel resection may be performed to treat gastrointestinal cancer, bowel ischemia, necrosis, or obstruction due to scar tissue, volvulus, and hernias. Some patients require ileostomy or colostomy after this procedure as alternative means of excretion. Complications of the procedure may include anastomotic leak or dehiscence, hernias, or adhesions causing partial or complete bowel obstruction. Depending on which part and how much of the intestines are removed, there may be digestive and metabolic challenges afterward, such as short bowel syndrome.

Bowel infarction or gangrenous bowel represents an irreversible injury to the intestine resulting from insufficient blood flow. It is considered a medical emergency because it can quickly result in life-threatening infection and death. Any cause of bowel ischemia, the earlier reversible form of injury, may ultimately lead to infarction if uncorrected. The causes of bowel ischemia or infarction include primary vascular causes and other causes of bowel obstruction.
Duodenal atresia is the congenital absence or complete closure of a portion of the lumen of the duodenum. It causes increased levels of amniotic fluid during pregnancy (polyhydramnios) and intestinal obstruction in newborn babies. Newborns present with bilious or non-bilous vomiting within the first 24 to 48 hours after birth, typically after their first oral feeding. Radiography shows a distended stomach and distended duodenum, which are separated by the pyloric valve, a finding described as the double-bubble sign.

Intestinal ischemia is a medical condition in which injury to the large or small intestine occurs due to not enough blood supply. It can come on suddenly, known as acute intestinal ischemia, or gradually, known as chronic intestinal ischemia. The acute form of the disease often presents with sudden severe abdominal pain and is associated with a high risk of death. The chronic form typically presents more gradually with abdominal pain after eating, unintentional weight loss, vomiting, and fear of eating.

Ladd's bands, sometimes called bands of Ladd, are fibrous stalks of peritoneal tissue that attach the cecum to the retroperitoneum in the right lower quadrant (RLQ). Obstructing Ladd's Bands are associated with malrotation of the intestine, a developmental disorder in which the cecum is found in the right upper quadrant (RUQ), instead of its normal anatomical position in the RLQ. Ladd's bands then pass over the second part of the duodenum, causing extrinsic compression and obstruction. This clinically manifests as poor feeding and bilious vomiting in neonates. Screening can be performed with an upper GI series. The most severe complication of malrotation is midgut volvulus, in which the mesenteric base twists around the superior mesenteric artery, compromising intestinal perfusion, leading to bowel necrosis.
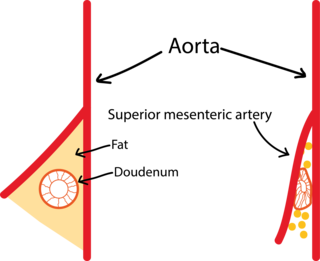
Superior mesenteric artery (SMA) syndrome is a gastro-vascular disorder in which the third and final portion of the duodenum is compressed between the abdominal aorta (AA) and the overlying superior mesenteric artery. This rare, potentially life-threatening syndrome is typically caused by an angle of 6–25° between the AA and the SMA, in comparison to the normal range of 38–56°, due to a lack of retroperitoneal and visceral fat. In addition, the aortomesenteric distance is 2–8 millimeters, as opposed to the typical 10–20. However, a narrow SMA angle alone is not enough to make a diagnosis, because patients with a low BMI, most notably children, have been known to have a narrow SMA angle with no symptoms of SMA syndrome.

William Edwards Ladd was an American surgeon, and is commonly regarded as one of the founders of pediatric surgery.
Neonatal bowel obstruction (NBO) or neonatal intestinal obstruction is the most common surgical emergency in the neonatal period. It may occur due to a variety of conditions and has an excellent outcome based on timely diagnosis and appropriate intervention.
In radiology, the double bubble sign is a feature of pediatric imaging seen on radiographs or prenatal ultrasound in which two air filled bubbles are seen in the abdomen, representing two discontiguous loops of bowel in a proximal, or 'high,' small bowel obstruction. The finding is typically pathologic, and implies either duodenal atresia, duodenal web, annular pancreas, or on occasion midgut volvulus, a distinction that requires close clinical correlation and, in most cases, surgical intervention.
