
The outer ear, external ear, or auris externa is the external part of the ear, which consists of the auricle and the ear canal. It gathers sound energy and focuses it on the eardrum.

Anotia describes a rare congenital deformity that involves the complete absence of the auricle, the outer projected portion of the ear, and narrowing or absence of the ear canal. This contrasts with microtia, in which a small part of the auricle is present. Anotia and microtia may occur unilaterally or bilaterally. This deformity results in conductive hearing loss, deafness.

An ear is the organ that enables hearing and body balance using the vestibular system. In mammals, the ear is usually described as having three parts: the outer ear, the middle ear and the inner ear. The outer ear consists of the pinna and the ear canal. Since the outer ear is the only visible portion of the ear in most animals, the word "ear" often refers to the external part alone. The middle ear includes the tympanic cavity and the three ossicles. The inner ear sits in the bony labyrinth, and contains structures which are key to several senses: the semicircular canals, which enable balance and eye tracking when moving; the utricle and saccule, which enable balance when stationary; and the cochlea, which enables hearing. The ear is a self cleaning organ through its relationship with earwax and the ear canals. The ears of vertebrates are placed somewhat symmetrically on either side of the head, an arrangement that aids sound localization.

The auricle or auricula is the visible part of the ear that is outside the head. It is also called the pinna, a term that is used more in zoology.

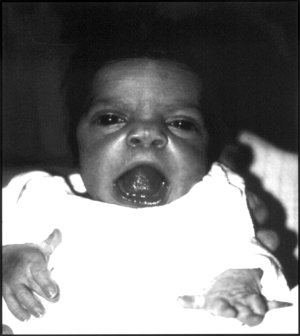
Treacher Collins syndrome (TCS) is a genetic disorder characterized by deformities of the ears, eyes, cheekbones, and chin. The degree to which a person is affected, however, may vary from mild to severe. Complications may include breathing problems, problems seeing, cleft palate, and hearing loss. Those affected generally have normal intelligence.

Conductive hearing loss (CHL) occurs when there is a problem transferring sound waves anywhere along the pathway through the outer ear, tympanic membrane (eardrum), or middle ear (ossicles). If a conductive hearing loss occurs in conjunction with a sensorineural hearing loss, it is referred to as a mixed hearing loss. Depending upon the severity and nature of the conductive loss, this type of hearing impairment can often be treated with surgical intervention or pharmaceuticals to partially or, in some cases, fully restore hearing acuity to within normal range. However, cases of permanent or chronic conductive hearing loss may require other treatment modalities such as hearing aid devices to improve detection of sound and speech perception.
Otoplasty is a procedure for correcting the deformities and defects of the auricle, whether these defects are congenital conditions or caused by trauma. Otoplastic surgeons may reshape, move, or augment the cartilaginous support framework of the auricle to correct these defects.
Unilateral hearing loss (UHL) is a type of hearing impairment where there is normal hearing in one ear and impaired hearing in the other ear.
Atresia is a condition in which an orifice or passage in the body is closed or absent.

Hemifacial microsomia (HFM) is a congenital disorder that affects the development of the lower half of the face, most commonly the ears, the mouth and the mandible. It usually occurs on one side of the face, but both sides are sometimes affected. If severe, it may result in difficulties in breathing due to obstruction of the trachea—sometimes even requiring a tracheotomy. With an incidence in the range of 1:3500 to 1:4500, it is the second most common birth defect of the face, after cleft lip and cleft palate. HFM shares many similarities with Treacher Collins syndrome.

A bone-anchored hearing aid (BAHA) is a type of hearing aid based on bone conduction. It is primarily suited for people who have conductive hearing losses, unilateral hearing loss, single-sided deafness and people with mixed hearing losses who cannot otherwise wear 'in the ear' or 'behind the ear' hearing aids. They are more expensive than conventional hearing aids, and their placement involves invasive surgery which carries a risk of complications, although when complications do occur, they are usually minor.
Robinow syndrome is an extremely rare genetic disorder characterized by short-limbed dwarfism, abnormalities in the head, face, and external genitalia, as well as vertebral segmentation. The disorder was first described in 1969 by human geneticist Meinhard Robinow, along with physicians Frederic N. Silverman and Hugo D. Smith, in the American Journal of Diseases of Children. By 2002, over 100 cases had been documented and introduced into medical literature.
Hearing loss with craniofacial syndromes is a common occurrence. Many of these multianomaly disorders involve structural malformations of the outer or middle ear, making a significant hearing loss highly likely.
Amastia refers to a rare clinical anomaly in which both internal breast tissue and the visible nipple are absent on one or both sides. It affects both men and women. Amastia can be either isolated or comorbid with other syndromes, such as ectodermal dysplasia, Syndactyly and lipoatrophic diabetes. This abnormality can be classified into various types, and each could result from different pathologies. Amastia differs from amazia and athelia. Amazia is the absence of one or both mammary glands but the nipples remain present, and athelia is the absence of one or both nipples, but the mammary gland remains.
Burt Brent is a retired reconstructive plastic surgeon best known for his work in reconstructing the absent outer ear. He built upon the techniques of his mentor, Dr. Radford Tanzer of the Mary Hitchcock Clinic at Dartmouth Medical School and repaired ear defects in 1,800 patients, most of them children born with ear deformities such as microtia. He also reconstructed ears lost or due to some form of trauma.
A facial cleft is an opening or gap in the face, or a malformation of a part of the face. Facial clefts is a collective term for all sorts of clefts. All structures like bone, soft tissue, skin etc. can be affected. Facial clefts are extremely rare congenital anomalies. There are many variations of a type of clefting and classifications are needed to describe and classify all types of clefting. Facial clefts hardly ever occur isolated; most of the time there is an overlap of adjacent facial clefts.

Cryptotia is the condition where an ear appears to have its upper portion buried underneath the side of the head. The condition also involves underdeveloped scapha and antihelical crura. Cryptotia is also known as buried ear or hidden ear.
Cartilage conduction is a pathway by which sound signals are transmitted to the inner ear. In 2004, Hiroshi Hosoi discovered this pathway and named “cartilage conduction”. Hearing by cartilage conduction is distinct from conventional sound-conduction pathways, such as air or bone, because it is realized by touching a transducer on the aural cartilage and does not involve the vibration of the skull bone. Therefore, cartilage conduction is referred to as the “third auditory pathway”.
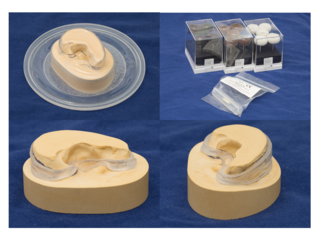
An auricular splint (AS) or ear splint is a custom-made medical device that is used to maintain auricular projection and dimensions following second stage auricular reconstruction. The AS is made from ethylene-vinyl acetate (EVA), which is typically used to make custom-made mouthguards and was developed by a team from Great Ormond Street Hospital in the United Kingdom.

Mandibulofacial dysostosis with microcephaly syndrome, also known as growth delay-intellectual disability-mandibulofacial dysostosis-microcephaly-cleft palate syndrome, mandibulofacial dysostosis, guion-almeida type, or simply as MFDM syndrome is a rare genetic disorder which is characterized by developmental delays, intellectual disabilities, and craniofacial dysmorphisms.



