
Cholesteatoma is a destructive and expanding growth consisting of keratinizing squamous epithelium in the middle ear and/or mastoid process. Cholesteatomas are not cancerous as the name may suggest, but can cause significant problems because of their erosive and expansile properties. This can result in the destruction of the bones of the middle ear (ossicles), as well as growth through the base of the skull into the brain. They often become infected and can result in chronically draining ears. Treatment almost always consists of surgical removal.
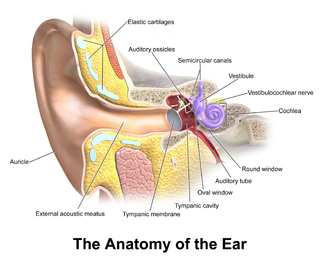
In the anatomy of humans and various other tetrapods, the eardrum, also called the tympanic membrane or myringa, is a thin, cone-shaped membrane that separates the external ear from the middle ear. Its function is to transmit sound from the air to the ossicles inside the middle ear, and then to the oval window in the fluid-filled cochlea. Hence, it ultimately converts and amplifies vibration in the air to vibration in cochlear fluid. The malleus bone bridges the gap between the eardrum and the other ossicles.

Otitis media is a group of inflammatory diseases of the middle ear. One of the two main types is acute otitis media (AOM), an infection of rapid onset that usually presents with ear pain. In young children this may result in pulling at the ear, increased crying, and poor sleep. Decreased eating and a fever may also be present. The other main type is otitis media with effusion (OME), typically not associated with symptoms, although occasionally a feeling of fullness is described; it is defined as the presence of non-infectious fluid in the middle ear which may persist for weeks or months often after an episode of acute otitis media. Chronic suppurative otitis media (CSOM) is middle ear inflammation that results in a perforated tympanic membrane with discharge from the ear for more than six weeks. It may be a complication of acute otitis media. Pain is rarely present. All three types of otitis media may be associated with hearing loss. If children with hearing loss due to OME do not learn sign language, it may affect their ability to learn.

The Eustachian tube, also called the auditory tube or pharyngotympanic tube, is a tube that links the nasopharynx to the middle ear, of which it is also a part. In adult humans, the Eustachian tube is approximately 35 mm (1.4 in) long and 3 mm (0.12 in) in diameter. It is named after the sixteenth-century Italian anatomist Bartolomeo Eustachi.

Conductive hearing loss (CHL) occurs when there is a problem transferring sound waves anywhere along the pathway through the outer ear, tympanic membrane (eardrum), or middle ear (ossicles). If a conductive hearing loss occurs in conjunction with a sensorineural hearing loss, it is referred to as a mixed hearing loss. Depending upon the severity and nature of the conductive loss, this type of hearing impairment can often be treated with surgical intervention or pharmaceuticals to partially or, in some cases, fully restore hearing acuity to within normal range. However, cases of permanent or chronic conductive hearing loss may require other treatment modalities such as hearing aid devices to improve detection of sound and speech perception.

Tympanoplasty is the surgical operation performed to reconstruct hearing mechanism of middle ear.

Ear pain, also known as earache or otalgia, is pain in the ear. Primary ear pain is pain that originates from the ear. Secondary ear pain is a type of referred pain, meaning that the source of the pain differs from the location where the pain is felt.
Patulous Eustachian tube is the name of a physical disorder where the Eustachian tube, which is normally closed, instead stays intermittently open. When this occurs, the person experiences autophony, the hearing of self-generated sounds. These sounds, such as one's own breathing, voice, and heartbeat, vibrate directly onto the ear drum and can create a "bucket on the head" effect, making it difficult for the patient to attend to environmental sounds. Patulous Eustachian tube is a form of Eustachian tube dysfunction, which is said to be present in about 1 percent of the general population.

Tympanostomy tube, also known as a grommet or myringotomy tube, is a small tube inserted into the eardrum in order to keep the middle ear aerated for a prolonged period of time, and to prevent the accumulation of fluid in the middle ear. The operation to insert the tube involves a myringotomy and is performed under local or general anesthesia. The tube itself is made in a variety of designs. The most commonly used type is shaped like a grommet. When it is necessary to keep the middle ear ventilated for a very long period, a T-shaped tube may be used, as these "T-tubes" can stay in place for 2–4 years. Materials used to construct the tube are most often plastics such as silicone or Teflon. Stainless steel tubes exist, but are no longer in frequent use.

Mastoiditis is the result of an infection that extends to the air cells of the skull behind the ear. Specifically, it is an inflammation of the mucosal lining of the mastoid antrum and mastoid air cell system inside the mastoid process. The mastoid process is the portion of the temporal bone of the skull that is behind the ear. The mastoid process contains open, air-containing spaces. Mastoiditis is usually caused by untreated acute otitis media and used to be a leading cause of child mortality. With the development of antibiotics, however, mastoiditis has become quite rare in developed countries where surgical treatment is now much less frequent and more conservative, unlike former times.
Otitis is a general term for inflammation in ear or ear infection, inner ear infection, middle ear infection of the ear, in both humans and other animals. When infection is present, it may be viral or bacterial. When inflammation is present due to fluid build up in the middle ear and infection is not present it is considered Otitis media with effusion. It is subdivided into the following:

Tympanometry is an acoustic evaluation of the condition of the middle ear eardrum and the conduction bones by creating variations of air pressure in the ear canal.

A perforated eardrum is a hole in the eardrum. It can be caused by infection, trauma, overpressure, inappropriate ear clearing, and changes in middle ear pressure. An otoscope can be used to view the eardrum to diagnose a perforation. Perforations may heal naturally or require surgery.
Myringoplasty is the closure of the perforation of pars tensa of the tympanic membrane. When myringoplasty is combined with removal of scar tissue, it is called tympanoplasty. The operation is performed with the patient supine and face turned to one side. The graft material most commonly used for the surgery is temporalis fascia. The tragal cartilage and tragal perichondrium are also used as the graft by some surgeons.

Tympanosclerosis is a condition caused by hyalinization and subsequent calcification of subepithelial connective tissue of the tympanic membrane and middle ear, sometimes resulting in a detrimental effect to hearing.

Tympanic membrane retraction describes a condition in which a part of the eardrum lies deeper within the ear than its normal position.
Endoscopic ear surgery (EES) is a minimally invasive alternative to traditional ear surgery and is defined as the use of the rigid endoscope, as opposed to a surgical microscope, to visualize the middle and inner ear during otologic surgery. During endoscopic ear surgery the surgeon holds the endoscope in one hand while working in the ear with the other. To allow this kind of single-handed surgery, different surgical instruments have to be used. Endoscopic visualization has improved due to high-definition video imaging and wide-field endoscopy, and being less invasive, EES is gaining importance as an adjunct to microscopic ear surgery.
Granular myringitis is a long term condition in which there is inflammation of the tympanic membrane in the ear and formation of granulation tissue within the tympanic membrane. It is a type of otitis externa.
Eustachian tube dysfunction (ETD) is a disorder where pressure abnormalities in the middle ear result in symptoms.
Middle ear barotrauma (MEBT), also known to underwater divers as ear squeeze and reverse ear squeeze, is an injury caused by a difference in pressure between the external ear canal and the middle ear. It is common in underwater divers and usually occurs when the diver does not equalise sufficiently during descent or, less commonly, on ascent. Failure to equalise may be due to inexperience or eustachian tube dysfunction, which can have many possible causes. Unequalised ambient pressure increase during descent causes a pressure imbalance between the middle ear air space and the external auditory canal over the eardrum, referred to by divers as ear squeeze, causing inward stretching, serous effusion and haemorrhage, and eventual rupture. During ascent internal over-pressure is normally passively released through the eustachian tube, but if this does not happen the volume expansion of middle ear gas will cause outward bulging, stretching and eventual rupture of the eardrum known to divers as reverse ear squeeze. This damage causes local pain and hearing loss. Tympanic rupture during a dive can allow water into the middle ear, which can cause severe vertigo from caloric stimulation. This may cause nausea and vomiting underwater, which has a high risk of aspiration of vomit or water, with possibly fatal consequences.
