In physiology, nociception, also nocioception; from Latin nocere 'to harm/hurt') is the sensory nervous system's process of encoding noxious stimuli. It deals with a series of events and processes required for an organism to receive a painful stimulus, convert it to a molecular signal, and recognize and characterize the signal to trigger an appropriate defensive response.

Empathy is generally described as the ability to take on another's perspective, to understand, feel, and possibly share and respond to their experience. There are more definitions of empathy that include but is not limited to social, cognitive, and emotional processes primarily concerned with understanding others. Often times, empathy is considered to be a broad term, and broken down into more specific concepts and types that include cognitive empathy, emotional empathy, somatic empathy, and spiritual empathy.

In the human brain, the anterior cingulate cortex (ACC) is the frontal part of the cingulate cortex that resembles a "collar" surrounding the frontal part of the corpus callosum. It consists of Brodmann areas 24, 32, and 33.

In neuroanatomy, the precuneus is the portion of the superior parietal lobule on the medial surface of each brain hemisphere. It is located in front of the cuneus. The precuneus is bounded in front by the marginal branch of the cingulate sulcus, at the rear by the parieto-occipital sulcus, and underneath by the subparietal sulcus. It is involved with episodic memory, visuospatial processing, reflections upon self, and aspects of consciousness.
A mirror neuron is a neuron that fires both when an organism acts and when the organism observes the same action performed by another. Thus, the neuron "mirrors" the behavior of the other, as though the observer were itself acting. Mirror neurons are not always physiologically distinct from other types of neurons in the brain; their main differentiating factor is their response patterns. By this definition, such neurons have been directly observed in humans and primate species, and in birds.
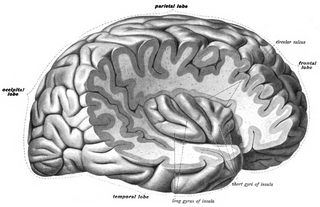
The insular cortex is a portion of the cerebral cortex folded deep within the lateral sulcus within each hemisphere of the mammalian brain.
Reduced affect display, sometimes referred to as emotional blunting or emotional numbing, is a condition of reduced emotional reactivity in an individual. It manifests as a failure to express feelings either verbally or nonverbally, especially when talking about issues that would normally be expected to engage emotions. In this condition, expressive gestures are rare and there is little animation in facial expression or vocal inflection. Additionally, reduced affect can be symptomatic of autism, schizophrenia, depression, post-traumatic stress disorder, depersonalization derealization disorder, schizoid personality disorder or brain damage. It may also be a side effect of certain medications.
Affective sensation is an occurrence of sensation accompanied with a strong compulsion to act on it. It refers, mostly in neuroscience, to the emotional sensibility in response to affective stimuli of a particular valence. It is transmitted via the spinothalamic tract through the spinal cord, and can be associated with reflex actions such as the scratch, gag, and withdrawal reflexes. Sensory processing in the brain interacts with behavioral choices, such as decisions to eat or to stop eating, in both healthy individuals and those with eating disorders.
The simulation theory of empathy holds that humans anticipate and make sense of the behavior of others by activating mental processes that, if they culminated in action, would produce similar behavior. This includes intentional behavior as well as the expression of emotions. The theory says that children use their own emotions to predict what others will do; we project our own mental states onto others.

Touch is perceiving the environment using skin. Specialized receptors in the skin send signals to the brain indicating light and soft pressure, hot and cold, body position and pain. It is a subset of the sensory nervous system, which also includes the visual, auditory, olfactory, gustatory and vestibular senses.
Mirror-touch synesthesia is a rare condition which causes individuals to experience a similar sensation in the same part or opposite part of the body that another person feels. For example, if someone with this condition were to observe someone touching their cheek, they would feel the same sensation on their own cheek. Synesthesia, in general, is described as a condition in which a concept or sensation causes an individual to experience an additional sensation or concept. Synesthesia is usually a developmental condition; however, recent research has shown that mirror touch synesthesia can be acquired after sensory loss following amputation.

Mindfulness has been defined in modern psychological terms as "paying attention to relevant aspects of experience in a nonjudgmental manner", and maintaining attention on present moment experience with an attitude of openness and acceptance. Meditation is a platform used to achieve mindfulness. Both practices, mindfulness and meditation, have been "directly inspired from the Buddhist tradition" and have been widely promoted by Jon Kabat-Zinn. Mindfulness meditation has been shown to have a positive impact on several psychiatric problems such as depression and therefore has formed the basis of mindfulness programs such as mindfulness-based cognitive therapy, mindfulness-based stress reduction and mindfulness-based pain management. The applications of mindfulness meditation are well established, however the mechanisms that underlie this practice are yet to be fully understood. Many tests and studies on soldiers with PTSD have shown tremendous positive results in decreasing stress levels and being able to cope with problems of the past, paving the way for more tests and studies to normalize and accept mindful based meditation and research, not only for soldiers with PTSD, but numerous mental inabilities or disabilities.

Tactile hallucination is the false perception of tactile sensory input that creates a hallucinatory sensation of physical contact with an imaginary object. It is caused by the faulty integration of the tactile sensory neural signals generated in the spinal cord and the thalamus and sent to the primary somatosensory cortex (SI) and secondary somatosensory cortex (SII). Tactile hallucinations are recurrent symptoms of neurological diseases such as schizophrenia, Parkinson's disease, Ekbom's syndrome and delirium tremens. Patients who experience phantom limb pains also experience a type of tactile hallucination. Tactile hallucinations are also caused by drugs such as cocaine and alcohol.

Interoception is the collection of senses providing information to the organism about the internal state of the body. This can be both conscious and subconscious. It encompasses the brain's process of integrating signals relayed from the body into specific subregions—like the brainstem, thalamus, insula, somatosensory, and anterior cingulate cortex—allowing for a nuanced representation of the physiological state of the body. This is important for maintaining homeostatic conditions in the body and, potentially, facilitating self-awareness.
Meditation and pain is the study of the physiological mechanisms underlying meditation—specifically its neural components—that implicate it in the reduction of pain perception.
Social cognitive neuroscience is the scientific study of the biological processes underpinning social cognition. Specifically, it uses the tools of neuroscience to study "the mental mechanisms that create, frame, regulate, and respond to our experience of the social world". Social cognitive neuroscience uses the epistemological foundations of cognitive neuroscience, and is closely related to social neuroscience. Social cognitive neuroscience employs human neuroimaging, typically using functional magnetic resonance imaging (fMRI). Human brain stimulation techniques such as transcranial magnetic stimulation and transcranial direct-current stimulation are also used. In nonhuman animals, direct electrophysiological recordings and electrical stimulation of single cells and neuronal populations are utilized for investigating lower-level social cognitive processes.
Network neuroscience is an approach to understanding the structure and function of the human brain through an approach of network science, through the paradigm of graph theory. A network is a connection of many brain regions that interact with each other to give rise to a particular function. Network Neuroscience is a broad field that studies the brain in an integrative way by recording, analyzing, and mapping the brain in various ways. The field studies the brain at multiple scales of analysis to ultimately explain brain systems, behavior, and dysfunction of behavior in psychiatric and neurological diseases. Network neuroscience provides an important theoretical base for understanding neurobiological systems at multiple scales of analysis.
Valeria Gazzola is an Italian neuroscientist, associate professor at the Faculty of Social and Behavioral Sciences at the University of Amsterdam (UvA) and member of the Young Academy of Europe. She is also a tenured department head at the Netherlands Institute for Neuroscience (NIN) in Amsterdam, where she leads her own research group and the Social Brain Lab together with neuroscientist Christian Keysers. She is a specialist in the neural basis of empathy and embodied cognition: Her research focusses on how the brain makes individuals sensitive to the actions and emotions of others and how this affects decision-making.
An empathy gap, sometimes referred to as an empathy bias, is a breakdown or reduction in empathy where it might otherwise be expected to occur. Empathy gaps may occur due to a failure in the process of empathizing or as a consequence of stable personality characteristics, and may reflect either a lack of ability or motivation to empathize.
Consoling touch is a pro-social behavior involving physical contact between a distressed individual and a caregiver. The physical contact, most commonly recognized in the form of a hand hold or embrace, is intended to comfort one or more of the participating individuals. Consoling touch is intended to provide consolation - to alleviate or lessen emotional or physical pain. This type of social support has been observed across species and cultures. Studies have found little difference in the applications of consoling touch, with minor differences in frequency occurrence across cultures. These findings suggest a degree of universality. It remains unclear whether the relationship between social touch and interpersonal emotional bonds reflect biologically driven or culturally normative behavior. Evidence of consoling touch in non-human primates, who embrace one another following distressing events, suggest a biological basis. Numerous studies of consoling touch in humans and animals unveil a consistent physiological response. An embrace from a friend, relative, or even stranger can trigger the release of oxytocin, dopamine, and serotonin into the bloodstream. These neurotransmitters are associated with positive mood, numerous health benefits, and longevity. Cortisol, a stress hormone, also decreases. Studies have found that the degree of intimacy and quality of relationship between consoler and the consoled mediates physiological effects. In other words, while subjects experience reduced cortisol levels while holding the hand of a stranger, they exhibit a larger effect when receiving comfort from a trusted friend, and greater still, when holding the hand of a high quality romantic partner.
