
Leishmania is a parasitic protozoan, a single-celled organism of the genus Leishmania that is responsible for the disease leishmaniasis. They are spread by sandflies of the genus Phlebotomus in the Old World, and of the genus Lutzomyia in the New World. At least 93 sandfly species are proven or probable vectors worldwide. Their primary hosts are vertebrates; Leishmania commonly infects hyraxes, canids, rodents, and humans.

Leishmaniasis is a wide array of clinical manifestations caused by protozoal parasites of the Trypanosomatida genus Leishmania. It is generally spread through the bite of phlebotomine sandflies, Phlebotomus and Lutzomyia, and occurs most frequently in the tropics and sub-tropics of Africa, Asia, the Americas, and southern Europe. The disease can present in three main ways: cutaneous, mucocutaneous, or visceral. The cutaneous form presents with skin ulcers, while the mucocutaneous form presents with ulcers of the skin, mouth, and nose. The visceral form starts with skin ulcers and later presents with fever, low red blood cell count, and enlarged spleen and liver.

Lieutenant-General Sir William Boog Leishman, was a Scottish pathologist and British Army medical officer. He was Director-General of Army Medical Services from 1923 to 1926.

Phlebotomus is a genus of "sand flies" in the Diptera family Psychodidae. In the past, they have sometimes been considered to belong in a separate family, Phlebotomidae, but this alternative classification has not gained wide acceptance.
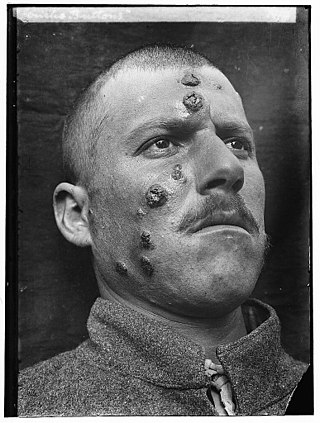
Cutaneous leishmaniasis is the most common form of leishmaniasis affecting humans. It is a skin infection caused by a single-celled parasite that is transmitted by the bite of a phlebotomine sand fly. There are about thirty species of Leishmania that may cause cutaneous leishmaniasis.

Visceral leishmaniasis (VL), also known as kala-azar or "black fever", is the most severe form of leishmaniasis and, without proper diagnosis and treatment, is associated with high fatality. Leishmaniasis is a disease caused by protozoan parasites of the genus Leishmania.
Rai Bahadur Sir Upendranath Brahmachari was a prominent Indian physician and scientist. In 1922, he synthesised urea-stibamine (carbostibamide) and demonstrated its effectiveness in treating kala-azar.
Pentavalent antimonials are a group of compounds used for the treatment of leishmaniasis. They are also called pentavalent antimony compounds.

The Drugs for Neglected Diseases initiative (DNDi) is a collaborative, patients' needs-driven, non-profit drug research and development (R&D) organization that is developing new treatments for neglected diseases, notably leishmaniasis, sleeping sickness, Chagas disease, malaria, filarial diseases, mycetoma, paediatric HIV, cryptococcal meningitis, hepatitis C, and dengue. DNDi's malaria activities were transferred to Medicines for Malaria Venture (MMV) in 2015.

Miltefosine, sold under the trade name Impavido among others, is a medication mainly used to treat leishmaniasis and free-living amoeba infections such as Naegleria fowleri and Balamuthia mandrillaris. This includes the three forms of leishmaniasis: cutaneous, visceral and mucosal. It may be used with liposomal amphotericin B or paromomycin. It is taken by mouth.
Antiparasitics are a class of medications which are indicated for the treatment of parasitic diseases, such as those caused by helminths, amoeba, ectoparasites, parasitic fungi, and protozoa, among others. Antiparasitics target the parasitic agents of the infections by destroying them or inhibiting their growth; they are usually effective against a limited number of parasites within a particular class. Antiparasitics are one of the antimicrobial drugs which include antibiotics that target bacteria, and antifungals that target fungi. They may be administered orally, intravenously or topically. Overuse or misuse of antiparasitics can lead to the development of antimicrobial resistance.

Canine leishmaniasis (LEESH-ma-NIGH-ah-sis) is a zoonotic disease caused by Leishmania parasites transmitted by the bite of an infected phlebotomine sandfly. There have been no documented cases of leishmaniasis transmission from dogs to humans. Canine leishmaniasis was first identified in Europe in 1903, and in 1940, 40% of all dogs in Rome were determined to be positive for leishmaniasis. Traditionally thought of as a disease only found near the Mediterranean basin, 2008 research claims new findings are evidence that canine leishmaniasis is currently expanding in continental climate areas of northwestern Italy, far from the recognized disease-endemic areas along the Mediterranean coasts. Cases of leishmaniasis began appearing in North America in 2000, and, as of 2008, Leishmania-positive foxhounds have been reported in 22 U.S. states and two Canadian provinces.
Leishmania donovani is a species of intracellular parasites belonging to the genus Leishmania, a group of haemoflagellate kinetoplastids that cause the disease leishmaniasis. It is a human blood parasite responsible for visceral leishmaniasis or kala-azar, the most severe form of leishmaniasis. It infects the mononuclear phagocyte system including spleen, liver and bone marrow. Infection is transmitted by species of sandfly belonging to the genus Phlebotomus in Old World and Lutzomyia in New World. The species complex it represents is prevalent throughout tropical and temperate regions including Africa, China, India, Nepal, southern Europe, Russia and South America. The species complex is responsible for thousands of deaths every year and has spread to 88 countries, with 350 million people at constant risk of infection and 0.5 million new cases in a year.

Leishmania tropica is a flagellate parasite and the cause of anthroponotic cutaneous leishmaniasis in humans. This parasite is restricted to Afro-Eurasia and is a common cause of infection in Afghanistan, Iran, Syria, Yemen, Algeria, Morocco, and northern India.
Leishmania braziliensis is a Leishmania species found in South America. It is associated with leishmaniasis.
Neglected tropical diseases in India are a group of bacterial, parasitic, viral, and fungal infections that are common in low income countries but receive little funding to address them. Neglected tropical diseases are common in India.
Kala azar in India refers to the special circumstances of the disease kala azar as it exists in India. Kala azar is a major health problem in India with an estimated 146,700 new cases per year as of 2012. In the disease a parasite causes sickness after migrating to internal organs such as the liver, spleen and bone marrow. If left untreated the disease almost always results in the death. Signs and symptoms include fever, weight loss, fatigue, anemia, and substantial swelling of the liver and spleen.

A Leishmaniasis vaccine is a vaccine which would prevent leishmaniasis. As of 2017, no vaccine for humans was available. Currently some effective leishmaniasis vaccines for dogs exist.
Shyam Sundar is an Indian academic and professor at Banaras Hindu University. He works on Infectious Diseases - Leishmaniasis & HIV/AIDS.

Ahmed Mohamed El HassanFRCP FTWAS was a Sudanese professor of pathology.
