Related Research Articles
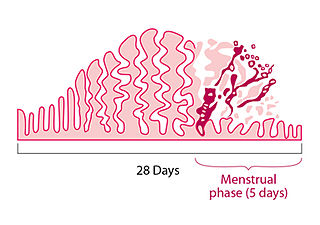
Menstruation is the regular discharge of blood and mucosal tissue from the inner lining of the uterus through the vagina. The menstrual cycle is characterized by the rise and fall of hormones. Menstruation is triggered by falling progesterone levels and is a sign that pregnancy has not occurred.

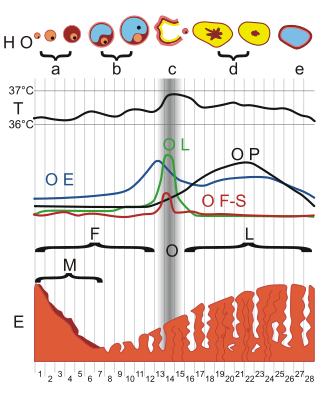
The menstrual cycle is a series of natural changes in hormone production and the structures of the uterus and ovaries of the female reproductive system that makes pregnancy possible. The ovarian cycle controls the production and release of eggs and the cyclic release of estrogen and progesterone. The uterine cycle governs the preparation and maintenance of the lining of the uterus (womb) to receive an embryo. These cycles are concurrent and coordinated, normally last between 21 and 35 days, with a median length of 28 days, and continue for about 30–45 years.
Amenorrhea is the absence of a menstrual period in a female who has reached reproductive age. Physiological states of amenorrhoea are seen, most commonly, during pregnancy and lactation (breastfeeding). Outside the reproductive years, there is absence of menses during childhood and after menopause.

A mood swing is an extreme or sudden change of mood. Such changes can play a positive part in promoting problem solving and in producing flexible forward planning, or be disruptive. When mood swings are severe, they may be categorized as part of a mental illness, such as bipolar disorder, where erratic and disruptive mood swings are a defining feature.
Dysmenorrhea, also known as period pain, painful periods or menstrual cramps, is pain during menstruation. Its usual onset occurs around the time that menstruation begins. Symptoms typically last less than three days. The pain is usually in the pelvis or lower abdomen. Other symptoms may include back pain, diarrhea or nausea.
Premenstrual dysphoric disorder (PMDD) is a mood disorder characterized by emotional, cognitive, and physical symptoms. PMDD causes significant distress or impairment in menstruating women during the luteal phase of the menstrual cycle. The symptoms occur in the luteal phase, improve within a few days after the onset of menses, and are minimal or absent in the week after menses. PMDD has a profound impact on a woman’s quality of life and dramatically increases the risk of suicidal ideation and even suicide attempts. Many women of reproductive age experience discomfort or mild mood changes prior to menstruation. However, 5–8% experience severe premenstrual syndrome causing significant distress or functional impairment. Within this population of reproductive age, some will meet the criteria for PMDD.
Anovulation is when the ovaries do not release an oocyte during a menstrual cycle. Therefore, ovulation does not take place. However, a woman who does not ovulate at each menstrual cycle is not necessarily going through menopause. Chronic anovulation is a common cause of infertility.

Katharina Daltonnée Kuipers was a British physician and pioneer in the research of premenstrual stress syndrome (PMS), coining the term, treating many women and testifying as an expert witness in influential court cases.
Premenstrual water retention is the buildup of additional water or fluid in the body. This phenomenon can be seen in various forms like increasing weight gain and swollen belly, legs, or ankles. Water retention is a symptom felt by some people of all backgrounds before their menstruation onset and was listed as one of the most common premenstrual symptoms in addition to cramping and back pain. There is a study that mentions the age effect being potentially linked to the intensity of symptoms, where the maximum symptom intensity was seen around age 35. This symptom, among others, have been connected to premenstrual syndrome (PMS), which is experienced by people days before their menstrual cycle begins. However, water retention itself can cause symptoms similar to those of PMS like body aches, headaches, and nausea. The actual duration of how long symptoms can last varies in length, from a few days to two weeks.
Breast pain is the symptom of discomfort in either one or both breasts. Pain in both breasts is often described as breast tenderness, is usually associated with the menstrual period and is not serious. Pain that involves only one part of a breast is more concerning, particularly if a hard mass or nipple discharge is also present.
A menstrual disorder is characterized as any abnormal condition with regards to a woman's menstrual cycle. There are many different types of menstrual disorders that vary with signs and symptoms, including pain during menstruation, heavy bleeding, or absence of menstruation. Normal variations can occur in menstrual patterns but generally menstrual disorders can also include periods that come sooner than 21 days apart, more than 3 months apart, or last more than 10 days in duration. Variations of the menstrual cycle are mainly caused by the immaturity of the hypothalamic-pituitary-ovarian (HPO) axis, and early detection and management is required in order to minimize the possibility of complications regarding future reproductive ability.
Psychoneuroendocrinology is the clinical study of hormone fluctuations and their relationship to human behavior. It may be viewed from the perspective of psychiatry, where in certain mood disorders, there are associated neuroendocrine or hormonal changes affecting the brain. It may also be viewed from the perspective of endocrinology, where certain endocrine disorders can be associated with negative health outcomes and psychiatric illness. Brain dysfunctions associated with the hypothalamus-pituitary-adrenal axis HPA axis can affect the endocrine system, which in turn can result in physiological and psychological symptoms. This complex blend of psychiatry, psychology, neurology, biochemistry, and endocrinology is needed to comprehensively understand and treat symptoms related to the brain, endocrine system (hormones), and psychological health..
Ovarian diseases refer to diseases or disorders of the ovary.
The classification of all headaches, including migraines, is organized by the International Headache Society, and published in the International Classification of Headache Disorders (ICHD). The current version, the ICHD-3 beta, was published in 2013.
Menstrual leave is a type of leave where a person may have the option to take paid or unpaid leave from their employment if they are menstruating and are unable to go to work because of this. Throughout its history, menstrual leave has been associated with controversy and discrimination against men, with very few countries enacting policies. In these countries, menstrual leave is still associated with low uptake. It is seen by some as a criticism of women's work efficiency or as sexism against men. Supporters of menstrual leave policies compare its function to that of maternity leave and view it as a promoter of gender equality.
Women's reproductive health in the United States refers to the set of physical, mental, and social issues related to the health of women in the United States. It includes the rights of women in the United States to adequate sexual health, available contraception methods, and treatment for sexually transmitted diseases. The prevalence of women's health issues in American culture is inspired by second-wave feminism in the United States. As a result of this movement, women of the United States began to question the largely male-dominated health care system and demanded a right to information on issues regarding their physiology and anatomy. The U.S. government has made significant strides to propose solutions, like creating the Women's Health Initiative through the Office of Research on Women's Health in 1991. However, many issues still exist related to the accessibility of reproductive healthcare as well as the stigma and controversy attached to sexual health, contraception, and sexually transmitted diseases.
Menstrual suppression refers to the practice of using hormonal management to stop or reduce menstrual bleeding. In contrast to surgical options for this purpose, such as hysterectomy or endometrial ablation, hormonal methods to manipulate menstruation are reversible.
Menstrual migraine is the term used to describe both true menstrual migraines and menstrually related migraines. About 7%–14% of women have migraines only at the time of menstruation. These are called true menstrual migraines. Most female migraineurs experience migraine attacks throughout the menstruation cycle with an increased number perimenstrually, these are referred to as menstrually related or menstrually triggered migraine.
Sleep problems in women can manifest at various stages of their life cycle. Both subjective and objective data indicate that women are at an increased risk of experiencing different types of sleeping problems during different life stages. Factors such as hormonal changes, aging, psycho-social aspects, physical and psychological conditions, and the presence of sleeping disorders can disrupt women's sleep. Research supports the presence of disturbed sleep during the menstrual cycle, pregnancy, postpartum period, and menopausal transition. The relationship between sleep and women's psychological well-being suggests that the underlying causes of sleep disturbances are often multi-factorial throughout a woman's lifespan.
Menstruation can have a notable impact on mental health, with some individuals experiencing mood disturbances and psychopathological symptoms during their menstrual cycle. Menstruation involves hormonal fluctuations and physiological changes in the body, which can affect a person's mood and psychological state. Many individuals report experiencing mood swings, irritability, anxiety, and even depression in the days leading up to their menstrual period. This cluster of symptoms is often referred to as premenstrual syndrome (PMS). For some individuals, the psychopathological symptoms associated with menstruation can be severe and debilitating, leading to a condition known as premenstrual dysphoric disorder (PMDD). PMDD is characterized by intense mood disturbances, cognitive, and somatic symptoms, which occur in a cyclical pattern linked to the menstrual cycle. In addition to PMDD, menstruation can exacerbate existing mental health conditions. The complex relationship between menstruation and mental well-being has garnered increased attention in both scientific research and public discourse.
References
- 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 "Premenstrual syndrome (PMS) fact sheet". Office on Women's Health. December 23, 2014. Archived from the original on 28 June 2015. Retrieved 23 June 2015.
- 1 2 3 4 5 6 7 8 9 10 11 12 13 Biggs, WS; Demuth, RH (15 October 2011). "Premenstrual syndrome and premenstrual dysphoric disorder". American Family Physician. 84 (8): 918–24. PMID 22010771.
- 1 2 3 4 5 6 7 8 9 10 11 12 13 Dickerson, Lori M.; Mazyck, Pamela J.; Hunter, Melissa H. (2003). "Premenstrual Syndrome". American Family Physician. 67 (8): 1743–52. PMID 12725453. Archived from the original on 2008-05-13.
- 1 2 3 4 5 6 7 8 9 Gudipally, Pratyusha R.; Sharma, Gyanendra K. (2022), "Premenstrual Syndrome", StatPearls, Treasure Island (FL): StatPearls Publishing, PMID 32809533 , retrieved 2023-01-31,
Premenstrual syndrome (PMS) encompasses clinically significant somatic and psychological manifestations during the luteal phase of the menstrual cycle, leading to substantial distress and impairment in functional capacity.
- 1 2 3 Mishra, Sanskriti; Elliott, Harold; Marwaha, Raman (2022), "Premenstrual Dysphoric Disorder", StatPearls, Treasure Island (FL): StatPearls Publishing, PMID 30335340 , retrieved 2023-01-31,
While some discomfort prior to menses is quite common, premenstrual syndrome (PMS) includes the subset of women who experience symptoms that are severe enough to impact daily activities and functioning.
- 1 2 3 "Premenstrual syndrome (PMS) | Office on Women's Health". www.womenshealth.gov. Retrieved 14 November 2022.
- 1 2 3 Tiranini L, Nappi RE (2022). "Recent advances in understanding/management of premenstrual dysphoric disorder/premenstrual syndrome". Fac Rev. 11: 11. doi: 10.12703/r/11-11 . PMC 9066446 . PMID 35574174.
- 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 King, Sally (2020), Bobel, Chris; Winkler, Inga T.; Fahs, Breanne; Hasson, Katie Ann (eds.), "Premenstrual Syndrome (PMS) and the Myth of the Irrational Female", The Palgrave Handbook of Critical Menstruation Studies, Singapore: Palgrave Macmillan, pp. 287–302, doi: 10.1007/978-981-15-0614-7_23 , ISBN 978-981-15-0613-0, PMID 33347177, S2CID 226733948 , retrieved 2023-01-31
- ↑ "Merck Manual Professional - Menstrual Abnormalities". November 2005. Archived from the original on 2007-02-12. Retrieved 2007-02-02.
- ↑ "MayoClinic.com: Premenstrual syndrome (PMS): Signs and symptoms". MayoClinic.com. 2006-10-27. Archived from the original on 2007-01-25. Retrieved 2007-02-02.
- ↑ Myra S., Hunter (2007). Psychological Challenges in Obstetrics and Gynecology. Springer. pp. 255–262. ISBN 978-1-84628-807-4.
- ↑ "Premenstrual Syndrome (PMS) - Gynecology and Obstetrics". MSD Manual Professional Edition. Retrieved 12 November 2022.
- ↑ Connolly, Moira (November 2001). "Premenstrual syndrome: an update on definitions, diagnosis and management". Advances in Psychiatric Treatment. 7 (6): 469–477. doi: 10.1192/apt.7.6.469 .
- ↑ "Depression in women" (PDF). Retrieved 11 November 2022.
- 1 2 3 4 5 Hutner, M.D, Lucy A.; Catapano, M.D., Ph.D., Lisa A.; Nagle-Yang, M.D., Sarah M.; Williams, M.D, Katherine E.; Osborne, M.D., Lauren M. (2021-12-07). Textbook of Women's Reproductive Mental Health. American Psychiatric Pub. pp. 173–174. ISBN 978-1-61537-306-2.
{{cite book}}: CS1 maint: multiple names: authors list (link) - ↑ "Water retention: Relieve this premenstrual symptom". Mayo Clinic. Archived from the original on 25 September 2011. Retrieved 20 September 2011.
- 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 Bieber, Eric J.; Sanfilippo, Joseph S.; Horowitz, Ira R.; Shafi, Mahmood I. (2015-04-23). Clinical Gynecology. Cambridge University Press. pp. 37–41. ISBN 978-1-107-04039-7.
- ↑ Ford, O; Lethaby, A; Roberts, H; Mol, BW (14 March 2012). "Progesterone for premenstrual syndrome". The Cochrane Database of Systematic Reviews. 2012 (3): CD003415. doi:10.1002/14651858.CD003415.pub4. PMC 7154383 . PMID 22419287.
- ↑ Marjoribanks, Jane; Brown, Julie; O'Brien, Patrick Michael Shaughn; Wyatt, Katrina (Jun 7, 2013). "Selective serotonin reuptake inhibitors for premenstrual syndrome" (PDF). The Cochrane Database of Systematic Reviews. 2013 (6): CD001396. doi:10.1002/14651858.CD001396.pub3. PMC 7073417 . PMID 23744611.
- ↑ Roca, CA; Schmidt, PJ; Rubinow, DR (1999). "A follow-up study of premenstrual syndrome". The Journal of Clinical Psychiatry. 60 (11): 763–6. doi:10.4088/JCP.v60n1108. PMID 10584765.
- ↑ Gershenson, David M.; Lentz, Gretchen M.; Valea, Fidel A.; Lobo, Rogerio A. (2021-05-08). Comprehensive Gynecology. Elsevier Health Sciences. p. 297. ISBN 978-0-323-79078-9.
Breast pain is typically divided into cyclic pain, related to the menstrual cycle, and noncyclic pain. Cyclic pain is diffuse and bilateral and most commonly associated with fibrocystic changes.
- ↑ "LifeWatch - Women's Health - Women's Reproductive Health: PMS". Archived from the original on 2009-02-10. Retrieved 2008-01-13.
- ↑ Lane, Darina (2011-07-20). "The Curse of PMS" (PDF). Evening Echo . Thomas Crosbie Holdings. p. 11. Archived from the original (PDF) on 2013-12-05. Retrieved 2012-06-03.
- ↑ Furchtgott-Roth, Diana; Stolba, Christine (2001). The feminist dilemma: when success is not enough (PDF). Washington, D.C: AEI Press. pp. 23–24. ISBN 978-0-8447-4129-1.
- ↑ Tsang, T.L. (2015) 'Article 1: "A fair chance for the girls": discourse on women's health and higher education in late nineteenth century America', American Educational History Journal, 42(1-2), 137+, available: https://link.gale.com/apps/doc/A437059646/AONE?u=mlin_oweb&sid=googleScholar&xid=3b3d1b1e [accessed 04 Mar 2024].
- ↑ Greene, Raymond and Katharina D. Dalton. (1953). "The Premenstrual Syndrome". British Medical Journal. 1 (4818): 1007–14. doi:10.1136/bmj.1.4818.1007. PMC 2016383 . PMID 13032605.
- 1 2 Markens, Susan (1996). "The Problematic of 'Experience': A Political and Cultural Critique of PMS". Gender & Society. 10 (1): 42–58. doi:10.1177/089124396010001004. JSTOR 189552. S2CID 145424718.
- ↑ Figert, Anne E. (1995). "The Three Faces of PMS: The Professional, Gendered, and Scientific Structuring of a Psychiatric Disorder". Social Problems. 42 (1): 56–73. doi:10.1525/sp.1995.42.1.03x0455m. JSTOR 3097005.
- 1 2 Carol Tavris, The Mismeasure of Woman (New York: Simon & Schuster, 1992), 142–144.
- 1 2 Bieber, Eric J.; Sanfilippo, Joseph S.; Horowitz, Ira R.; Shafi, Mahmood I. (2015-04-23). Clinical Gynecology. Cambridge University Press. pp. 37–41. ISBN 978-1-107-04039-7.