Related Research Articles

Cognitive behavioral therapy (CBT) is a psycho-social intervention that aims to reduce symptoms of various mental health conditions, primarily depression and anxiety disorders. Cognitive behavioral therapy is one of the most effective means of treatment for substance abuse and co-occurring mental health disorders. CBT focuses on challenging and changing cognitive distortions and their associated behaviors to improve emotional regulation and develop personal coping strategies that target solving current problems. Though it was originally designed to treat depression, its uses have been expanded to include many issues and the treatment of many mental health conditions, including anxiety, substance use disorders, marital problems, ADHD, and eating disorders. CBT includes a number of cognitive or behavioral psychotherapies that treat defined psychopathologies using evidence-based techniques and strategies.
Psychoanalysis is a set of theories and therapeutic techniques that deal in part with the unconscious mind, and which together form a method of treatment for mental disorders. The discipline was established in the early 1890s by Sigmund Freud, whose work stemmed partly from the clinical work of Josef Breuer and others. Freud developed and refined the theory and practice of psychoanalysis until his death in 1939. In an encyclopedia article, he identified the cornerstones of psychoanalysis as "the assumption that there are unconscious mental processes, the recognition of the theory of repression and resistance, the appreciation of the importance of sexuality and of the Oedipus complex." Freud's colleagues Alfred Adler and Carl Gustav Jung developed offshoots of psychoanalysis which they called individual psychology (Adler) and analytical psychology (Jung), although Freud himself wrote a number of criticisms of them and emphatically denied that they were forms of psychoanalysis. Psychoanalysis was later developed in different directions by neo-Freudian thinkers, such as Erich Fromm, Karen Horney, and Harry Stack Sullivan.
Psychotherapy is the use of psychological methods, particularly when based on regular personal interaction, to help a person change behavior, increase happiness, and overcome problems. Psychotherapy aims to improve an individual's well-being and mental health, to resolve or mitigate troublesome behaviors, beliefs, compulsions, thoughts, or emotions, and to improve relationships and social skills. Numerous types of psychotherapy have been designed either for individual adults, families, or children and adolescents. Certain types of psychotherapy are considered evidence-based for treating some diagnosed mental disorders; other types have been criticized as pseudoscience.
Group psychotherapy or group therapy is a form of psychotherapy in which one or more therapists treat a small group of clients together as a group. The term can legitimately refer to any form of psychotherapy when delivered in a group format, including art therapy, cognitive behavioral therapy or interpersonal therapy, but it is usually applied to psychodynamic group therapy where the group context and group process is explicitly utilized as a mechanism of change by developing, exploring and examining interpersonal relationships within the group.
Occupational therapists (OTs) are health care professionals specializing in occupational therapy and occupational science. OTs and occupational therapy assistants (OTAs) use scientific bases and a holistic perspective to promote a person's ability to fulfill their daily routines and roles. OTs have training in the physical, psychological, and social aspects of human functioning deriving from an education grounded in anatomical and physiological concepts, and psychological perspectives. They enable individuals across the lifespan by optimizing their abilities to perform activities that are meaningful to them ("occupations"). Human occupations include activities of daily living, work/vocation, play, education, leisure, rest and sleep, and social participation.
Transactional analysis is a psychoanalytic theory and method of therapy wherein social interactions are analyzed to determine the ego state of the communicator as a basis for understanding behavior. In transactional analysis, the communicator is taught to alter the ego state as a way to solve emotional problems. The method deviates from Freudian psychoanalysis which focuses on increasing awareness of the contents of subconsciously held ideas. Eric Berne developed the concept and paradigm of transactional analysis in the late 1950s.
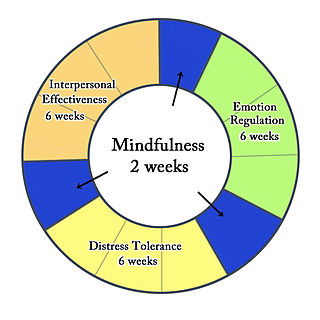
Dialectical behavior therapy (DBT) is an evidence-based psychotherapy that began with efforts to treat personality disorders and interpersonal conflicts. Evidence suggests that DBT can be useful in treating mood disorders and suicidal ideation as well as for changing behavioral patterns such as self-harm and substance use. DBT evolved into a process in which the therapist and client work with acceptance and change-oriented strategies and ultimately balance and synthesize them—comparable to the philosophical dialectical process of thesis and antithesis, followed by synthesis.
Gestalt therapy is a form of psychotherapy that emphasizes personal responsibility and focuses on the individual's experience in the present moment, the therapist–client relationship, the environmental and social contexts of a person's life, and the self-regulating adjustments people make as a result of their overall situation. It was developed by Fritz Perls, Laura Perls and Paul Goodman in the 1940s and 1950s, and was first described in the 1951 book Gestalt Therapy.
Dance/movement therapy (DMT) in USA and Australia or dance movement psychotherapy (DMP) in the UK is the psychotherapeutic use of movement and dance to support intellectual, emotional, and motor functions of the body. As a modality of the creative arts therapies, DMT looks at the correlation between movement and emotion.
Art therapy is a distinct discipline that incorporates creative methods of expression through visual art media. Art therapy, as a creative arts therapy profession, originated in the fields of art and psychotherapy and may vary in definition.
Psychodynamic psychotherapy and psychoanalytic psychotherapy are two categories of psychological therapies. Their main purpose is revealing the unconscious content of a client's psyche in an effort to alleviate psychic tension, which is inner conflict within the mind that was created in a situation of extreme stress or emotional hardship, often in the state of distress. The terms "psychoanalytic psychotherapy" and "psychodynamic psychotherapy" are often used interchangeably, but a distinction can be made in practice: though psychodynamic psychotherapy largely relies on psychoanalytical theory, it employs substantially shorter treatment periods than traditional psychoanalytical therapies. Psychodynamic psychotherapy is evidence-based; the effectiveness of psychoanalysis and its relationship to facts is disputed.

Play therapy refers to a range of methods of capitalising on children's natural urge to explore and harnessing it to meet and respond to the developmental and later also their mental health needs. It is also used for forensic or psychological assessment purposes where the individual is too young or too traumatised to give a verbal account of adverse, abusive or potentially criminal circumstances in their life.

William Ronald Dodds Fairbairn FRSE was a Scottish psychiatrist, psychoanalyst and a central figure in the development of the Object Relations Theory of psychoanalysis. He usually used, and was known as and referred to as, "W. Ronald D. Fairbairn".
Resistance, in psychoanalysis, refers to the client's defence mechanisms that emerge from unconscious content coming to fruition through process. Resistance is the repression of unconscious drives from integration into conscious awareness.
Psychological resistance, also known as psychological resistance to change, is the phenomenon often encountered in clinical practice in which patients either directly or indirectly exhibit paradoxical opposing behaviors in presumably a clinically initiated push and pull of a change process. In other words, the concept of psychological resistance is that patients are likely to resist physician suggestions to change behavior or accept certain treatments regardless of whether that change will improve their condition. It impedes the development of authentic, reciprocally nurturing experiences in a clinical setting. Psychological resistance can manifest in various ways, such as denying the existence or severity of a problem, rationalizing or minimizing one's responsibility for it, rejecting or distrusting the therapist's or consultant's suggestions, withholding or distorting information, or sabotaging the treatment process. It is established that the common source of resistances and defenses is shame. This and similar negative attitudes may be the result of social stigmatization of a particular condition, such as psychological resistance towards insulin treatment of diabetes.
Child psychotherapy, or mental health interventions for children refers to the psychological treatment of various mental disorders diagnosed in children and adolescents. The therapeutic techniques developed for younger age ranges specialize in prioritizing the relationship between the child and the therapist. The goal of maintaining positive therapist-client relationships is typically achieved using therapeutic conversations and can take place with the client alone, or through engagement with family members.
The developmental needs meeting strategy (DNMS) is a psychotherapy approach developed by Shirley Jean Schmidt. It is designed to treat adults with psychological trauma wounds and with attachment wounds. The DNMS is an ego state therapy based on the assumption that the degree to which developmental needs were not adequately met is the degree to which a client may be stuck in childhood. This model aims to identify ego states that are stuck in the past and help them get unstuck by remediating those unmet developmental needs. The processing starts with the DNMS therapist guiding a patient to mobilize three internal Resource ego states: a Nurturing Adult Self, a Protective Adult Self, and a Spiritual Core Self. The therapist then guides these three Resources to gently help wounded child ego states get unstuck from the past by meeting their unmet developmental needs, helping them process through painful emotions, and by establishing an emotional bond. The relationship wounded child parts have with these Resources is considered the primary agent for change.
Schema therapy was developed by Jeffrey E. Young for use in treatment of personality disorders and chronic DSM Axis I disorders, such as when patients fail to respond or relapse after having been through other therapies. Schema therapy is an integrative psychotherapy combining theory and techniques from previously existing therapies, including cognitive behavioral therapy, psychoanalytic object relations theory, attachment theory, and Gestalt therapy.
Psychotherapy discontinuation, also known as unilateral termination, patient dropout, and premature termination, is a patient's decision to stop mental health treatment before they have received an adequate number of sessions. In the United States, the prevalence of patient dropout is estimated to be between 40–60% over the course of treatment however, the overwhelming majority of patients will drop after two sessions. An exhaustive meta-analysis of 146 studies in Western countries showed that the mean dropout rate is 34.8% with a wide range of 10.3% to 81.0%. The studies from the US (n = 85) had a dropout rate of 37.9% (range: 33.0% to 43.0%).
Co-therapy or conjoint therapy is a kind of psychotherapy conducted with more than one therapist present. This kind of therapy is especially applied during couple therapy. Carl Whitaker and Virginia Satir are credited as the founders of co-therapy. Co-therapy dates back to the early twentieth century in Vienna, where psychoanalytic practices were first taking place. It was originally named "multiple therapy" by Alfred Alder, and later introduced separately as "co-therapy" in the 1940s. Co-therapy began with two therapists of differing abilities, one essentially learning from the other, and providing the opportunity to hear feedback on their work.
References
- 1 2 3 4 5 6 Moroney, Margaret (1989). "Comparison of 5 methods". Transactional Analysis Journal. 19: 35–41. doi:10.1177/036215378901900106.
- ↑ Carroll RT (2011), "Psychotherapies, New Age", The Skeptic's Dictionary: A Collection of Strange Beliefs, Amusing Deceptions, and Dangerous Delusions, John Wiley & Sons, p. 317, ISBN 978-1-118-04563-3
- 1 2 Munilla, Horacio (1982). "Defective parenting and reparenting". Transactional Analysis Journal. 12 (3): 181–184. doi:10.1177/036215378201200302.
- ↑ Lankford, Valerie (1988). "The parent ego state from a reparenting perspective". Transactional Analysis Journal. 18: 47–50. doi:10.1177/036215378801800108.
- ↑ Lankford, Valerie (1998). "A reparented daughter's perspective". Transactional Analysis Journal. 28: 31–34. doi:10.1177/036215379802800108.
- ↑ Osnes, Russell (1974). "Spot reparenting". Transactional Analysis Journal. 4 (3): 40–46. doi:10.1177/036215377400400308.
- ↑ James, Muriel (1998). "Self-reparenting and redecision". Transactional Analysis Journal. 28: 16–19. doi:10.1177/036215379802800106.
- ↑ Rumney, Avis (1985). "Growing up and getting dependency needs met as an adult: Reparenting in anorexia nervosa". Transactional Analysis Journal. 15: 55–61. doi:10.1177/036215378501500110.
- ↑ Schiff, Jacqui (1977). "Biochemical evidence of cure in schizophrenics". Transactional Analysis Journal. 7 (2): 178–182. doi:10.1177/036215377700700217.
- ↑ Wissink, Lilian (1994). "A validation of transactional analysis in increasing self-esteem among participants in a self-reparenting program". Transactional Analysis Journal. 24 (3): 189–196. doi:10.1177/036215379402400306.
- ↑ Gayol, Gloria (1995). "Self-reparenting with female delinquents in jail". Transactional Analysis Journal. 25 (3): 208–210. doi:10.1177/036215379502500303.
- 1 2 3 4 Weiss, Laurie (1994). "Ethics of parenting and reparenting". Transactional Analysis Journal. 24: 57–59. doi:10.1177/036215379402400110.
- 1 2 3 Jacobs, Alan (1994). "Theory as ideology: Reparenting and thought reform". Transactional Analysis Journal. 24: 39–55. doi:10.1177/036215379402400108.
- ↑ Woods, Ken (1998). "The Danger of Sadomasochism in the Reparenting of Psychotics". Transactional Analysis Journal. 28: 48–54. doi:10.1177/036215379802800111.