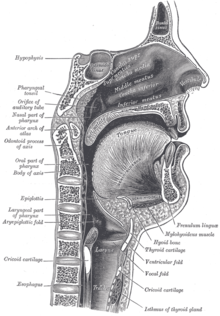
The larynx, commonly called the voice box, is an organ in the top of the neck involved in breathing, producing sound and protecting the trachea against food aspiration. The opening of larynx into pharynx known as the laryngeal inlet is about 4–5 centimeters in diameter. The larynx houses the vocal cords, and manipulates pitch and volume, which is essential for phonation. It is situated just below where the tract of the pharynx splits into the trachea and the esophagus. The word 'larynx' comes from the Ancient Greek word lárunx ʻlarynx, gullet, throat.ʼ
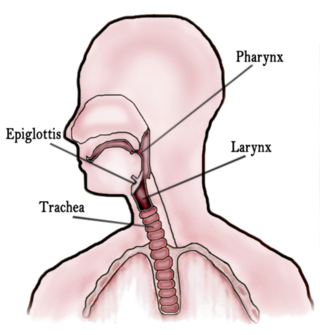
In vertebrate anatomy, the throat is the front part of the neck, internally positioned in front of the vertebrae. It contains the pharynx and larynx. An important section of it is the epiglottis, separating the esophagus from the trachea (windpipe), preventing food and drinks being inhaled into the lungs. The throat contains various blood vessels, pharyngeal muscles, the nasopharyngeal tonsil, the tonsils, the palatine uvula, the trachea, the esophagus, and the vocal cords. Mammal throats consist of two bones, the hyoid bone and the clavicle. The "throat" is sometimes thought to be synonymous for the fauces.

The esophagus or oesophagus, colloquially known also as the food pipe, food tube, or gullet, is an organ in vertebrates through which food passes, aided by peristaltic contractions, from the pharynx to the stomach. The esophagus is a fibromuscular tube, about 25 cm (10 in) long in adults, that travels behind the trachea and heart, passes through the diaphragm, and empties into the uppermost region of the stomach. During swallowing, the epiglottis tilts backwards to prevent food from going down the larynx and lungs. The word oesophagus is from Ancient Greek οἰσοφάγος (oisophágos), from οἴσω (oísō), future form of φέρω + ἔφαγον.
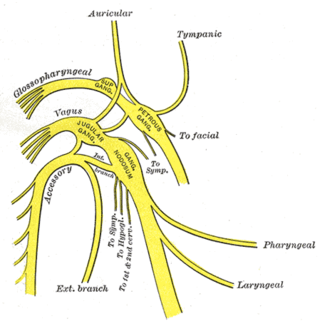
The glossopharyngeal nerve, also known as the ninth cranial nerve, cranial nerve IX, or simply CN IX, is a cranial nerve that exits the brainstem from the sides of the upper medulla, just anterior to the vagus nerve. Being a mixed nerve (sensorimotor), it carries afferent sensory and efferent motor information. The motor division of the glossopharyngeal nerve is derived from the basal plate of the embryonic medulla oblongata, whereas the sensory division originates from the cranial neural crest.

The epiglottis is a leaf-shaped flap in the throat that prevents food and water from entering the trachea and the lungs. It stays open during breathing, allowing air into the larynx. During swallowing, it closes to prevent aspiration of food into the lungs, forcing the swallowed liquids or food to go along the esophagus toward the stomach instead. It is thus the valve that diverts passage to either the trachea or the esophagus.
The pharyngeal reflex or gag reflex is a reflex muscular contraction of the back of the throat, evoked by touching the roof of the mouth, back of the tongue, area around the tonsils, uvula, and back of the throat. It, along with other aerodigestive reflexes such as reflexive pharyngeal swallowing, prevents objects in the oral cavity from entering the throat except as part of normal swallowing and helps prevent choking, and is a form of coughing. The pharyngeal reflex is different from the laryngeal spasm, which is a reflex muscular contraction of the vocal cords.
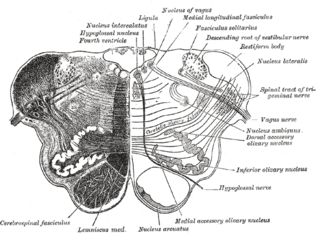
The nucleus ambiguus is a group of large motor neurons, situated deep in the medullary reticular formation named by Jacob Clarke. The nucleus ambiguus contains the cell bodies of neurons that innervate the muscles of the soft palate, pharynx, and larynx which are associated with speech and swallowing. As well as motor neurons, the nucleus ambiguus contains preganglionic parasympathetic neurons which innervate postganglionic parasympathetic neurons in the heart.
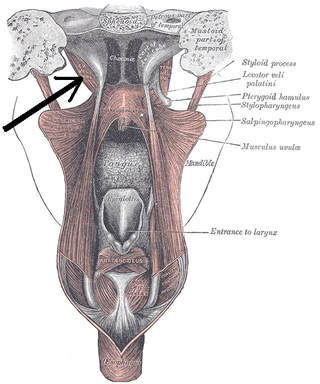
The levator veli palatini is a muscle of the soft palate and pharynx. It is innervated by the vagus nerve via its pharyngeal plexus. During swallowing, it contracts, elevating the soft palate to help prevent food from entering the nasopharynx.

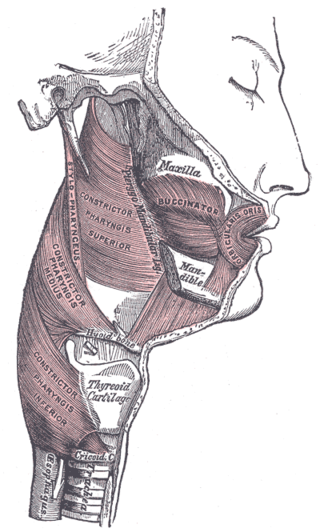
The middle pharyngeal constrictor is a fan-shaped muscle located in the neck. It is one of three pharyngeal constrictor muscles. It is smaller than the inferior pharyngeal constrictor muscle.

The inferior pharyngeal constrictor muscle is a skeletal muscle of the neck. It is the thickest of the three outer pharyngeal muscles. It arises from the sides of the cricoid cartilage and the thyroid cartilage. It is supplied by the vagus nerve. It is active during swallowing, and partially during breathing and speech. It may be affected by Zenker's diverticulum.

The superior pharyngeal constrictor muscle is a quadrilateral muscle of the pharynx. It is the uppermost and thinnest of the three pharyngeal constrictors.

The stylopharyngeus muscle is a muscle in the head. It originates from the temporal styloid process. Some of its fibres insert onto the thyroid cartilage, while others end by intermingling with proximal structures. It is innervated by the glossopharyngeal nerve. It acts to elevate the larynx and pharynx, and dilate the pharynx, thus facilitating swallowing.

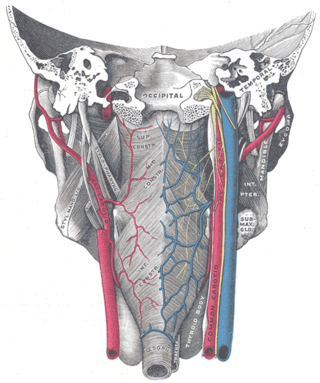
The inferior thyroid artery is an artery in the neck. It arises from the thyrocervical trunk and passes upward, in front of the vertebral artery and longus colli muscle. It then turns medially behind the carotid sheath and its contents, and also behind the sympathetic trunk, the middle cervical ganglion resting upon the vessel.
The superior laryngeal nerve is a branch of the vagus nerve. It arises from the middle of the inferior ganglion of vagus nerve and additionally also receives a sympathetic branch from the superior cervical ganglion.
Oropharyngeal dysphagia is the inability to empty material from the oropharynx into the esophagus as a result of malfunction near the esophagus. Oropharyngeal dysphagia manifests differently depending on the underlying pathology and the nature of the symptoms. Patients with dysphagia can experience feelings of food sticking to their throats, coughing and choking, weight loss, recurring chest infections, or regurgitation. Depending on the underlying cause, age, and environment, dysphagia prevalence varies. In research including the general population, the estimated frequency of oropharyngeal dysphagia has ranged from 2 to 16 percent.
The pharyngeal muscles are a group of muscles that form the pharynx, which is posterior to the oral cavity, determining the shape of its lumen, and affecting its sound properties as the primary resonating cavity.
The pharyngeal plexus is a nerve plexus located upon the outer surface of the pharynx. It contains a motor component, a sensory component, and sympathetic component.
Presbyphagia refers to characteristic changes in the swallowing mechanism of otherwise healthy older adults. Although age-related changes place older adults at risk swallowing disorders, an older adult's swallow is not necessarily an impaired swallow. Clinicians are becoming more aware of the need to distinguish among swallowing disorders, presbyphagia and other related diagnoses in order to avoid over diagnosing and over treating presbyphagia. Older adults are more vulnerable and with the increased threat of acute illnesses, medications and any number of age-related conditions, they can cross the line from having a healthy older swallow to being dysphagic.

The pharynx is the part of the throat behind the mouth and nasal cavity, and above the esophagus and trachea. It is found in vertebrates and invertebrates, though its structure varies across species. The pharynx carries food to the esophagus and air to the larynx. The flap of cartilage called the epiglottis stops food from entering the larynx.

The human digestive system consists of the gastrointestinal tract plus the accessory organs of digestion. Digestion involves the breakdown of food into smaller and smaller components, until they can be absorbed and assimilated into the body. The process of digestion has three stages: the cephalic phase, the gastric phase, and the intestinal phase.