The sensory nervous system is a part of the nervous system responsible for processing sensory information. A sensory system consists of sensory neurons, neural pathways, and parts of the brain involved in sensory perception and interoception. Commonly recognized sensory systems are those for vision, hearing, touch, taste, smell, balance and visceral sensation. Sense organs are transducers that convert data from the outer physical world to the realm of the mind where people interpret the information, creating their perception of the world around them.

Afferent nerve fibers are axons of sensory neurons that carry sensory information from sensory receptors to the central nervous system. Many afferent projections arrive at a particular brain region.
A mechanoreceptor, also called mechanoceptor, is a sensory receptor that responds to mechanical pressure or distortion. Mechanoreceptors are innervated by sensory neurons that convert mechanical pressure into electrical signals that, in animals, are sent to the central nervous system.

The spinothalamic tract is a part of the anterolateral system or the ventrolateral system, a sensory pathway to the thalamus. From the ventral posterolateral nucleus in the thalamus, sensory information is relayed upward to the somatosensory cortex of the postcentral gyrus.
The dorsal column–medial lemniscus pathway (DCML) is a sensory pathway of the central nervous system that conveys sensations of fine touch, vibration, two-point discrimination, and proprioception (position) from the skin and joints. It transmits information from the body to the primary somatosensory cortex in the postcentral gyrus of the parietal lobe of the brain. The pathway receives information from sensory receptors throughout the body, and carries this in nerve tracts in the white matter of the dorsal column of the spinal cord to the medulla, where it is continued in the medial lemniscus, on to the thalamus and relayed from there through the internal capsule and transmitted to the somatosensory cortex. The name dorsal-column medial lemniscus comes from the two structures that carry the sensory information: the dorsal columns of the spinal cord, and the medial lemniscus in the brainstem.
Stereognosis is the ability to perceive and recognize the form of an object in the absence of visual and auditory information, by using tactile information to provide cues from texture, size, spatial properties, and temperature, etc. In humans, this sense, along with tactile spatial acuity, vibration perception, texture discrimination and proprioception, is mediated by the dorsal column-medial lemniscus pathway of the central nervous system. Stereognosis tests determine whether or not the parietal lobe of the brain is intact. Typically, these tests involved having the patient identify common objects placed in their hand without any visual cues. Stereognosis is a higher cerebral associative cortical function.
Sensory substitution is a change of the characteristics of one sensory modality into stimuli of another sensory modality.
A topographic map is the ordered projection of a sensory surface, like the retina or the skin, or an effector system, like the musculature, to one or more structures of the central nervous system. Topographic maps can be found in all sensory systems and in many motor systems.
Cutaneous innervation refers to the area of the skin which is supplied by a specific cutaneous nerve.

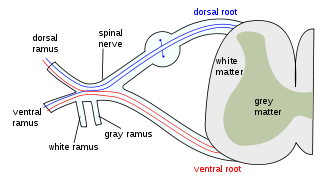
Group C nerve fibers are one of three classes of nerve fiber in the central nervous system (CNS) and peripheral nervous system (PNS). The C group fibers are unmyelinated and have a small diameter and low conduction velocity, whereas Groups A and B are myelinated. Group C fibers include postganglionic fibers in the autonomic nervous system (ANS), and nerve fibers at the dorsal roots. These fibers carry sensory information.
Pallesthesia, or vibratory sensation, is the ability to perceive vibration. This sensation, often conducted through skin and bone, is usually generated by mechanoreceptors such as Pacinian corpuscles, Merkel disk receptors, and tactile corpuscles. All of these receptors stimulate an action potential in afferent nerves found in various layers of the skin and body. The afferent neuron travels to the spinal column and then to the brain where the information is processed. Damage to the peripheral nervous system or central nervous system can result in a decline or loss of pallesthesia.

Two-point discrimination (2PD) is the ability to discern that two nearby objects touching the skin are truly two distinct points, not one. It is often tested with two sharp points during a neurological examination and is assumed to reflect how finely innervated an area of skin is.

In physiology, the somatosensory system is the network of neural structures in the brain and body that produce the perception of touch, as well as temperature (thermoception), body position (proprioception), and pain. It is a subset of the sensory nervous system, which also represents visual, auditory, olfactory, and gustatory stimuli.

Proprioception, also referred to as kinaesthesia, is the sense of self-movement, force, and body position. It is sometimes described as the "sixth sense".
A somatosensory disorder is an impairment of the somatosensory system.
Amorphosynthesis, also called a hemi-sensory deficit, is a neuropsychological condition in which a patient experiences unilateral inattention to sensory input. This phenomenon is frequently associated with damage to the right cerebral hemisphere resulting in severe sensory deficits that are observed on the contralesional (left) side of the body. A right-sided deficit is less commonly observed and the effects are reported to be temporary and minor. Evidence suggests that the right cerebral hemisphere has a dominant role in attention and awareness to somatic sensations through ipsilateral and contralateral stimulation. In contrast, the left cerebral hemisphere is activated only by contralateral stimuli. Thus, the left and right cerebral hemispheres exhibit redundant processing to the right-side of the body and a lesion to the left cerebral hemisphere can be compensated by the ipsiversive processes of the right cerebral hemisphere. For this reason, right-sided amorphosynthesis is less often observed and is generally associated with bilateral lesions.

Cross modal plasticity is the adaptive reorganization of neurons to integrate the function of two or more sensory systems. Cross modal plasticity is a type of neuroplasticity and often occurs after sensory deprivation due to disease or brain damage. The reorganization of the neural network is greatest following long-term sensory deprivation, such as congenital blindness or pre-lingual deafness. In these instances, cross modal plasticity can strengthen other sensory systems to compensate for the lack of vision or hearing. This strengthening is due to new connections that are formed to brain cortices that no longer receive sensory input.
Many types of sense loss occur due to a dysfunctional sensation process, whether it be ineffective receptors, nerve damage, or cerebral impairment. Unlike agnosia, these impairments are due to damages prior to the perception process.

Tactile hallucination is the false perception of tactile sensory input that creates a hallucinatory sensation of physical contact with an imaginary object. It is caused by the faulty integration of the tactile sensory neural signals generated in the spinal cord and the thalamus and sent to the primary somatosensory cortex (SI) and secondary somatosensory cortex (SII). Tactile hallucinations are recurrent symptoms of neurological diseases such as schizophrenia, Parkinson's disease, Ekbom's syndrome and delerium tremens. Patients who experience phantom limb pains also experience a type of tactile hallucination. Tactile hallucinations are also caused by drugs such as cocaine and alcohol.
Tactile induced analgesia is the phenomenon where concurrent touch and pain on the skin reduces the intensity of pain that is felt.