Related Research Articles

Myalgia is the medical term for muscle pain. Myalgia is a symptom of many diseases. The most common cause of acute myalgia is the overuse of a muscle or group of muscles; another likely cause is viral infection, especially when there has been no trauma.

Tietze syndrome is a benign inflammation of one or more of the costal cartilages. It was first described in 1921 by German surgeon Alexander Tietze and was subsequently named after him. The condition is characterized by tenderness and painful swelling of the anterior (front) chest wall at the costochondral, sternocostal, or sternoclavicular junctions. Tietze syndrome affects the true ribs and has a predilection for the 2nd and 3rd ribs, commonly affecting only a single joint.
Fibromyalgia is a medical condition which causes chronic widespread pain, accompanied by fatigue, waking unrefreshed, and cognitive symptoms. Other symptoms include headaches, lower abdominal pain or cramps, and depression. People with fibromyalgia can also experience insomnia and a general hypersensitivity.

Chest pain is pain or discomfort in the chest, typically the front of the chest. It may be described as sharp, dull, pressure, heaviness or squeezing. Associated symptoms may include pain in the shoulder, arm, upper abdomen, or jaw, along with nausea, sweating, or shortness of breath. It can be divided into heart-related and non-heart-related pain. Pain due to insufficient blood flow to the heart is also called angina pectoris. Those with diabetes or the elderly may have less clear symptoms.

Costochondritis, also known as chest wall pain syndrome or costosternal syndrome, is a benign inflammation of the upper costochondral and sternocostal joints. 90% of patients are affected in multiple ribs on a single side, typically at the 2nd to 5th ribs. Chest pain, the primary symptom of costochondritis, is considered a symptom of a medical emergency, making costochondritis a common presentation in the emergency department. One study found costochondritis was responsible for 30% of patients with chest pain in an emergency department setting.
A diagnosis of exclusion or by exclusion is a diagnosis of a medical condition reached by a process of elimination, which may be necessary if presence cannot be established with complete confidence from history, examination or testing. Such elimination of other reasonable possibilities is a major component in performing a differential diagnosis.
Reactive airway disease (RAD) is an informal label that physicians apply to patients with symptoms similar to those of asthma. An exact definition of the condition does not exist. Individuals who are typically labeled as having RAD generally have a history of wheezing, coughing, dyspnea, and production of sputum that may or may not be caused by asthma. Symptoms may also include, but are not limited to, coughing, shortness of breath, excess mucus in the bronchial tube, swollen mucous membrane in the bronchial tube, and/or hypersensitive bronchial tubes. Physicians most commonly label patients with RAD when they are hesitant about formally diagnosing a patient with asthma, which is most prevalent in the pediatric setting. While some physicians may use RAD and asthma synonymously, there is controversy over this usage.
Da Costa's syndrome, also known as soldier's heart among other names, was a syndrome or a set of symptoms similar to those of heart disease. These include fatigue upon exertion, shortness of breath, palpitations, sweating, chest pain, and sometimes orthostatic intolerance. It was originally thought to be a cardiac condition, and treated with a predecessor to modern cardiac drugs. In modern times, it is believed to represent several unrelated disorders, some of which have a known medical basis.
Medically unexplained physical symptoms are symptoms for which a treating physician or other healthcare providers have found no medical cause, or whose cause remains contested. In its strictest sense, the term simply means that the cause for the symptoms is unknown or disputed—there is no scientific consensus. Not all medically unexplained symptoms are influenced by identifiable psychological factors. However, in practice, most physicians and authors who use the term consider that the symptoms most likely arise from psychological causes. Typically, the possibility that MUPS are caused by prescription drugs or other drugs is ignored. It is estimated that between 15% and 30% of all primary care consultations are for medically unexplained symptoms. A large Canadian community survey revealed that the most common medically unexplained symptoms are musculoskeletal pain, ear, nose, and throat symptoms, abdominal pain and gastrointestinal symptoms, fatigue, and dizziness. The term MUPS can also be used to refer to syndromes whose etiology remains contested, including chronic fatigue syndrome, fibromyalgia, multiple chemical sensitivity and Gulf War illness.
Clouding of consciousness, also called brain fog or mental fog, occurs when a person is slightly less wakeful or aware than normal. They are less aware of time and their surroundings, and find it difficult to pay attention. People describe this subjective sensation as their mind being "foggy".

Clinical descriptions of ME/CFS vary. Different groups have produced sets of diagnostic criteria that share many similarities. The biggest differences between criteria are whether post-exertional malaise (PEM) is required, and the number of symptoms needed.

Medical diagnosis is the process of determining which disease or condition explains a person's symptoms and signs. It is most often referred to as a diagnosis with the medical context being implicit. The information required for a diagnosis is typically collected from a history and physical examination of the person seeking medical care. Often, one or more diagnostic procedures, such as medical tests, are also done during the process. Sometimes the posthumous diagnosis is considered a kind of medical diagnosis.
Functional disorders are a group of recognisable medical conditions which are due to changes to the functioning of the systems of the body rather than due to a disease affecting the structure of the body.
Myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS) is a debilitating long-term medical condition. People with ME/CFS experience delayed worsening of the illness after minor physical or mental activity, which is the hallmark symptom of the illness. Other core symptoms are a greatly reduced ability to do tasks that were previously routine, severe fatigue that does not improve much with rest, and sleep disturbances. Further common symptoms include dizziness or nausea when sitting or standing, along with memory and concentration issues and pain.
Kent Holtorf is an American physician and entrepreneur practicing in Los Angeles, California. He is a board examiner of the American Board of Anti-Aging Medicine (ABAAM), which is not recognized by established medical organizations. He is the founder and medical director of Holtorf Medical Group, a practice with five centers that offer treatment for conditions including fibromyalgia, adrenal fatigue, complex endocrine dysfunction, hypothyroidism, age management, chronic fatigue syndrome, low libido, chronic Lyme disease, migraines, PMS, perimenopause and menopause. His practice focuses on alternative therapies that are not recognised as effective. He has been criticized in the media for his controversial views on topics like bioidentical hormone replacement therapy and vaccines.
Chronic Lyme disease (CLD) is the name used by some people with non-specific symptoms, such as fatigue, muscle pain, and cognitive dysfunction to refer to their condition, even if there is no evidence that they had Lyme disease. Both the label and the belief that these people's symptoms are caused by this particular infection are generally rejected by medical professionals. Chronic Lyme disease is distinct from post-treatment Lyme disease syndrome, a set of lingering symptoms which may persist after successful antibiotic treatment of infection with Lyme-causing Borrelia bacteria, and which may have similar symptoms to CLD.

Chest pain in children is the pain felt in the chest by infants, children and adolescents. In most cases the pain is not associated with the heart. It is primarily identified by the observance or report of pain by the infant, child or adolescent by reports of distress by parents or caregivers. Chest pain is not uncommon in children. Many children are seen in ambulatory clinics, emergency departments and hospitals and cardiology clinics. Most often there is a benign cause for the pain for most children. Some have conditions that are serious and possibly life-threatening. Chest pain in pediatric patients requires careful physical examination and a detailed history that would indicate the possibility of a serious cause. Studies of pediatric chest pain are sparse. It has been difficult to create evidence-based guidelines for evaluation.
The term functional somatic syndrome (FSS) refers to a group of chronic diagnoses with no identifiable organic cause. This term was coined by Hemanth Samkumar. It encompasses disorders such as fibromyalgia, chronic widespread pain, temporomandibular disorder, irritable bowel syndrome, lower back pain, tension headache, atypical face pain, non-cardiac chest pain, insomnia, palpitation, dyspepsia and dizziness. General overlap exists between this term, somatization and somatoform. The status of ME/CFS as a functional somatic syndrome is contested. Although the aetiology remains unclear, there are consistent findings of biological abnormalities, and major health bodies such as the NAM, WHO, and NIH, classify it as an organic disease.
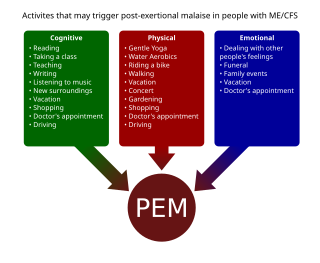
Post-exertional malaise (PEM), sometimes referred to as post-exertional symptom exacerbation (PESE) or post-exertional neuroimmune exhaustion (PENE), is a worsening of symptoms that occurs after minimal exertion. It is the hallmark symptom of myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS) and common in long COVID and fibromyalgia PEM is often severe enough to be disabling, and is triggered by ordinary activities that healthy people tolerate. Typically, it begins 12–48 hours after the activity that triggers it, and lasts for days, but this is highly variable and may persist much longer. Management of PEM is symptom-based, and patients are recommended to pace their activities to avoid triggering PEM.
Idiopathic chronic fatigue (ICF) or chronic idiopathic fatigue or insufficient/idiopathic fatigue is a term used for cases of unexplained fatigue that have lasted at least six consecutive months and which do not meet the criteria for Myalgic Encephalomyelitis/chronic fatigue syndrome. Such fatigue is widely understood to have a profound effect on the lives of patients who experience it.
References
- ↑ Smith TL (2003). "Vasomotor rhinitis is not a wastebasket diagnosis". Arch. Otolaryngol. Head Neck Surg. 129 (5): 584–7. doi:10.1001/archotol.129.5.584. PMID 12759275.
- ↑ Rauh SM, Schoetz DJ, Roberts PL, Murray JJ, Coller JA, Veidenheimer MC (1991). "Pouchitis--is it a wastebasket diagnosis?". Dis. Colon Rectum. 34 (8): 685–9. doi:10.1007/BF02050351. PMID 1649737. S2CID 20265782.
- ↑ Napodano RJ (1977). "The functional heart murmur: a wastebasket diagnosis". J Fam Pract. 4 (4): 637–9. PMID 853276.
- ↑ GAMBILL EE (1960). "So-called mesenteric adenitis. A clinical entity or wastebasket diagnosis?". Minn Med. 43: 614–6. PMID 13703254.
- ↑ Eastman M (1978). "Senility: the 'diagnostic wastebasket'". Am Pharm. 18 (10): 53. doi:10.1016/S0160-3450(15)32615-5. PMID 696591.
- ↑ Freeman HJ (2008). "Refractory celiac disease and sprue-like intestinal disease". World J. Gastroenterol. 14 (6): 828–30. doi: 10.3748/wjg.14.828 . PMC 2687049 . PMID 18240339.
- ↑ Herndon RM (2006). "Multiple sclerosis mimics". Adv Neurol. 98: 161–6. PMID 16400833.
- 1 2 3 4 5 Barron H. Lerner, MD (25 March 2008). "When the Disease Eludes a Diagnosis". New York Times. Retrieved 2008-03-29.
For example, many patients with chest pain carry a diagnosis of costochondritis (inflammation of the chest wall bones) or gastroesophageal reflux (regurgitation of stomach acid into the esophagus). These are real conditions. But they tend to generate little interest from many physicians, who may refer to them as 'wastebasket diagnoses,' offered when nothing more serious has turned up. The frustration of patients who believe that the medical profession takes these types of ailments too lightly has led groups of them to form alliances to publicize their illnesses. Foremost among them are fibromyalgia, a syndrome involving muscular and other pains, and chronic fatigue syndrome...
- 1 2 3 4 5 6 7 8 9 10 Moldofsky, Harvey (2015), Chokroverty, Sudhansu; Billiard, Michel (eds.), "Nonrestorative Sleep, Musculoskeletal Pain, Fatigue in Rheumatic Disorders, and Allied Syndromes: A Historical Perspective", Sleep Medicine, New York, NY: Springer New York, pp. 423–431, doi:10.1007/978-1-4939-2089-1_48, ISBN 978-1-4939-2088-4, PMC 7122008 , retrieved 2024-05-01
- ↑ "Why You Should Never Settle for an IBS Diagnosis". Bella Lindemann. 2016-11-01. Retrieved 2023-07-08.
- ↑ "The Mysteries and Underdiagnosis of SIBO". Time. 2022-03-07. Retrieved 2023-07-08.
- ↑ Pfeffer, Glenn B.; Easley, Mark E.; Hintermann, Beat; Sands, Andrew K.; Younger, Alastair S. E. (2017-08-15). Operative Techniques: Foot and Ankle Surgery E-Book. Elsevier Health Sciences. p. 669. ISBN 978-0-323-51191-9.
...the wastebasket diagnosis of 'shin splints' which can be stress fractures, periostitis, or exertional compartment syndrome.
- ↑ Randall G. Fisher; Thomas G. Boyce; Hugh L. Moffet (2005). Moffet's Pediatric Infectious Diseases: A Problem-oriented Approach. Lippincott Williams & Wilkins. pp. 145–. ISBN 978-0-7817-2943-7.
- ↑ Chelimsky, Thomas C. 2009. “CHAPTER 9: Pain.” In Clinical Adult Neurology, 149–65. Demos Medical Publishing, LLC. ISBN 9781933864358.
- ↑ Stobb, Mike (2007). "Autism 'epidemic' largely fueled by special ed funding, shift in diagnosing".
The recent explosion of cases appears to be mostly caused by a surge in special education services for autistic children, and by a corresponding shift in what doctors call autism.
- ↑ Thompson, C.J.S. (January 24, 2003) [1928]. Quacks of Old London. Kessinger Publishing. p. 80. ISBN 978-0-7661-3609-0 . Retrieved February 11, 2012.
- ↑ Grossman, Anne Chotzinoff, Lisa Grossman Thomas, Patrick O'Brian (2000). Lobscouse & Spotted Dog: Which It's a Gastronomic Companion to the Aubrey. W. W. Norton & Company. pp. 249–250. ISBN 978-0-393-32094-7.
{{cite book}}: CS1 maint: multiple names: authors list (link) - ↑ Burke, Peter; Roy Porter (22 October 1987). The Social history of language. Cambridge University Press. pp. 89–90. ISBN 978-0-521-31763-4.
- ↑ Lerner, Barron H. (March 25, 2008). "When the Disease Eludes a Diagnosis (Published 2008)". The New York Times– via NYTimes.com.
- ↑ Servan-Schreiber, David; Tabas, Gary; Kolb, N. Randall (March 1, 2000). "Somatizing Patients: Part II. Practical Management". American Family Physician. 61 (5): 1423–8, 1431–2. PMID 10735347 – via www.aafp.org.