Related Research Articles

Asbestosis is long-term inflammation and scarring of the lungs due to asbestos fibers. Symptoms may include shortness of breath, cough, wheezing, and chest tightness. Complications may include lung cancer, mesothelioma, and pulmonary heart disease.

A granuloma is an aggregation of macrophages that forms in response to chronic inflammation. This occurs when the immune system attempts to isolate foreign substances that it is otherwise unable to eliminate. Such substances include infectious organisms including bacteria and fungi, as well as other materials such as foreign objects, keratin, and suture fragments.

Pulmonary alveolar proteinosis (PAP) is a rare lung disorder characterized by an abnormal accumulation of surfactant-derived lipoprotein compounds within the alveoli of the lung. The accumulated substances interfere with the normal gas exchange and expansion of the lungs, ultimately leading to difficulty breathing and a predisposition to developing lung infections. The causes of PAP may be grouped into primary, secondary, and congenital causes, although the most common cause is a primary autoimmune condition in an individual.

Interstitial lung disease (ILD), or diffuse parenchymal lung disease (DPLD), is a group of respiratory diseases affecting the interstitium and space around the alveoli of the lungs. It concerns alveolar epithelium, pulmonary capillary endothelium, basement membrane, and perivascular and perilymphatic tissues. It may occur when an injury to the lungs triggers an abnormal healing response. Ordinarily, the body generates just the right amount of tissue to repair damage, but in interstitial lung disease, the repair process is disrupted, and the tissue around the air sacs (alveoli) becomes scarred and thickened. This makes it more difficult for oxygen to pass into the bloodstream. The disease presents itself with the following symptoms: shortness of breath, nonproductive coughing, fatigue, and weight loss, which tend to develop slowly, over several months. The average rate of survival for someone with this disease is between three and five years. The term ILD is used to distinguish these diseases from obstructive airways diseases.

A chest radiograph, called a chest X-ray (CXR), or chest film, is a projection radiograph of the chest used to diagnose conditions affecting the chest, its contents, and nearby structures. Chest radiographs are the most common film taken in medicine.

Hypersensitivity pneumonitis (HP) or extrinsic allergic alveolitis (EAA) is a syndrome caused by the repetitive inhalation of antigens from the environment in susceptible or sensitized people. Common antigens include molds, bacteria, bird droppings, bird feathers, agricultural dusts, bioaerosols and chemicals from paints or plastics. People affected by this type of lung inflammation (pneumonitis) are commonly exposed to the antigens by their occupations, hobbies, the environment and animals. The inhaled antigens produce a hypersensitivity immune reaction causing inflammation of the airspaces (alveoli) and small airways (bronchioles) within the lung. Hypersensitivity pneumonitis may eventually lead to interstitial lung disease.

Lung abscess is a type of liquefactive necrosis of the lung tissue and formation of cavities containing necrotic debris or fluid caused by microbial infection.

Moslem Bahadori was an Iranian medical scientist, pathologist, and a university lecturer. In 1973, Bahadori along with Averill Abraham Liebow, reported the first case of plasma cell granuloma, a benign tumor of the lung.

Pneumonitis describes general inflammation of lung tissue. Possible causative agents include radiation therapy of the chest, exposure to medications used during chemo-therapy, the inhalation of debris, aspiration, herbicides or fluorocarbons and some systemic diseases. If unresolved, continued inflammation can result in irreparable damage such as pulmonary fibrosis.
Eosinophilic pneumonia is a disease in which an eosinophil, a type of white blood cell, accumulates in the lungs. These cells cause disruption of the normal air spaces (alveoli) where oxygen is extracted from the atmosphere. Several different kinds of eosinophilic pneumonia exist and can occur in any age group. The most common symptoms include cough, fever, difficulty breathing, and sweating at night. Eosinophilic pneumonia is diagnosed by a combination of characteristic symptoms, findings on a physical examination by a health provider, and the results of blood tests and X-rays. Prognosis is excellent once most eosinophilic pneumonia is recognized and treatment with corticosteroids is begun.

Lipoid pneumonia is a specific form of lung inflammation (pneumonia) that develops when lipids enter the bronchial tree. The disorder is sometimes called cholesterol pneumonia in cases where that lipid is a factor.
Lymphomatoid granulomatosis (LYG or LG) is a very rare lymphoproliferative disorder first characterized in 1972. Lymphomatoid means lymphoma-like and granulomatosis denotes the microscopic characteristic of the presence of granulomas with polymorphic lymphoid infiltrates and focal necrosis within it.
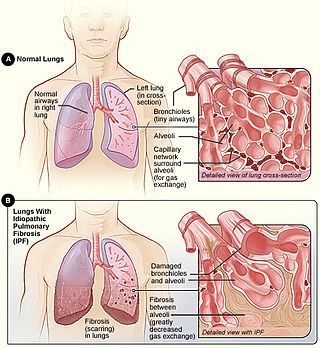
Idiopathic pulmonary fibrosis (IPF), or (formerly) fibrosing alveolitis, is a rare, progressive illness of the respiratory system, characterized by the thickening and stiffening of lung tissue, associated with the formation of scar tissue. It is a type of chronic scarring lung disease characterized by a progressive and irreversible decline in lung function. The tissue in the lungs becomes thick and stiff, which affects the tissue that surrounds the air sacs in the lungs. Symptoms typically include gradual onset of shortness of breath and a dry cough. Other changes may include feeling tired, and abnormally large and dome shaped finger and toenails. Complications may include pulmonary hypertension, heart failure, pneumonia or pulmonary embolism.
Henry D. Tazelaar is a lung, heart and transplant pathologist.

Usual interstitial pneumonia (UIP) is a form of lung disease characterized by progressive scarring of both lungs. The scarring (fibrosis) involves the pulmonary interstitium. UIP is thus classified as a form of interstitial lung disease.

Idiopathic interstitial pneumonia (IIP), or noninfectious pneumonia are a class of diffuse lung diseases. These diseases typically affect the pulmonary interstitium, although some also have a component affecting the airways. There are seven recognized distinct subtypes of IIP.

Benjamin Castleman was an American physician and pathologist best known for describing Castleman's disease, which is named after him. He was also one of the authors of the first case series on pulmonary alveolar proteinosis in a 1958 article in the New England Journal of Medicine. Castleman undertook clinicopathologic investigations of parathyroid disease and wrote several important papers on diseases of the thymus and mediastinum. He wrote, or collaborated in writing, over 100 scholarly papers on a variety of disorders.
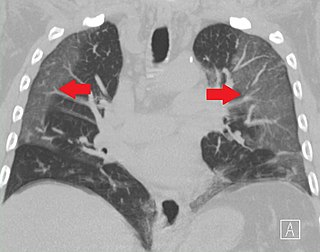
Ground-glass opacity (GGO) is a finding seen on chest x-ray (radiograph) or computed tomography (CT) imaging of the lungs. It is typically defined as an area of hazy opacification (x-ray) or increased attenuation (CT) due to air displacement by fluid, airway collapse, fibrosis, or a neoplastic process. When a substance other than air fills an area of the lung it increases that area's density. On both x-ray and CT, this appears more grey or hazy as opposed to the normally dark-appearing lungs. Although it can sometimes be seen in normal lungs, common pathologic causes include infections, interstitial lung disease, and pulmonary edema.

Lotte Strauss was a German-American pathologist.
Shields Warren was an American pathologist. He was among the first to study the pathology of radioactive fallout. Warren influenced and mentored Eleanor Josephine Macdonald, epidemiologist and cancer researcher.
References
- 1 2 3 4 5 6 Bloor, C. M. (September 1978). "In remembrance of Averill A. Liebow, March 31, 1911--May 31, 1978". The American Journal of Pathology. 92 (3): 577–580. ISSN 0002-9440. PMC 2018275 . PMID 356624.
- 1 2 3 "DR. AVERILL A. LIEBOW". The New York Times. 1978-06-02. ISSN 0362-4331 . Retrieved 2021-04-05.
- 1 2 3 Scarani, Paolo (2004-04-01). "The Pathologist and the Bomb: Averill A. Liebow in Hiroshima". International Journal of Surgical Pathology. 12 (2): 147–148. doi:10.1177/106689690401200208. ISSN 1066-8969. PMID 15173920. S2CID 30833501.
- ↑ "Dr. Averill A. Liebow Addresses the Mexican Academy of Medicine". library.ucsd.edu. 1969-01-13. Retrieved 2021-04-05.
- 1 2 "Collection: Averill A. Liebow Collection | Archives at Yale". archives.yale.edu. Retrieved 2021-04-05.
- 1 2 3 4 "1953-1954 Averill Abraham Liebow, USA (Austria)". www.iapcentral.org. Retrieved 2021-04-05.
- 1 2 3 4 Smith, G. J. (1981). "Averill Abraham Liebow: contributions to pulmonary pathology". The Yale Journal of Biology and Medicine. 54 (2): 139–146. ISSN 0044-0086. PMC 2595850 . PMID 7023079.
- ↑ Nicholson, Andrew G. (2008). "Interstitial Pneumonias". Dail and Hammar's Pulmonary Pathology. pp. 695–721. doi:10.1007/978-0-387-68792-6_19. ISBN 978-0-387-98395-0. PMC 7122677 .
- ↑ Kim, Dong Soon; Collard, Harold R.; King, Talmadge E. (June 2006). "Classification and Natural History of the Idiopathic Interstitial Pneumonias". Proceedings of the American Thoracic Society. 3 (4): 285–292. doi:10.1513/pats.200601-005TK. ISSN 1546-3222. PMC 2658683 . PMID 16738191.
- 1 2 3 4 5 6 Cummings, Mike (2015-08-05). "Chronicles of disaster: Hiroshima in the Yale University Library archives". YaleNews. Retrieved 2021-04-05.
- ↑ "Averill Abraham Liebow". www.whonamedit.com. Retrieved 2021-04-05.
| International | |
|---|---|
| National | |
| Other | |