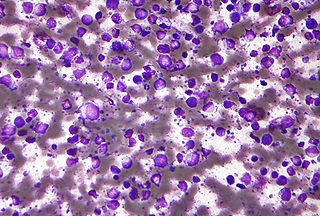
Primary effusion lymphoma (PEL) is classified as a diffuse large B cell lymphoma. It is a rare malignancy of plasmablastic cells that occurs in individuals that are infected with the Kaposi's sarcoma-associated herpesvirus. Plasmablasts are immature plasma cells, i.e. lymphocytes of the B-cell type that have differentiated into plasmablasts but because of their malignant nature do not differentiate into mature plasma cells but rather proliferate excessively and thereby cause life-threatening disease. In PEL, the proliferating plasmablastoid cells commonly accumulate within body cavities to produce effusions, primarily in the pleural, pericardial, or peritoneal cavities, without forming a contiguous tumor mass. In rare cases of these cavitary forms of PEL, the effusions develop in joints, the epidural space surrounding the brain and spinal cord, and underneath the capsule which forms around breast implants. Less frequently, individuals present with extracavitary primary effusion lymphomas, i.e., solid tumor masses not accompanied by effusions. The extracavitary tumors may develop in lymph nodes, bone, bone marrow, the gastrointestinal tract, skin, spleen, liver, lungs, central nervous system, testes, paranasal sinuses, muscle, and, rarely, inside the vasculature and sinuses of lymph nodes. As their disease progresses, however, individuals with the classical effusion-form of PEL may develop extracavitary tumors and individuals with extracavitary PEL may develop cavitary effusions.

T-cell lymphoma is a rare form of cancerous lymphoma affecting T-cells. Lymphoma arises mainly from the uncontrolled proliferation of T-cells and can become cancerous.
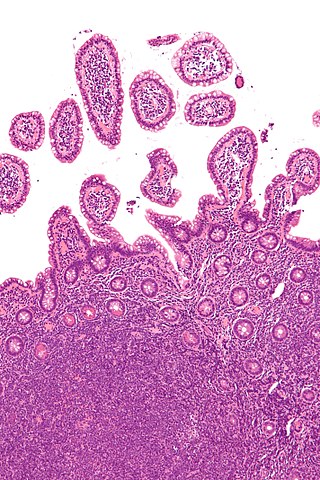
Diffuse large B-cell lymphoma (DLBCL) is a cancer of B cells, a type of lymphocyte that is responsible for producing antibodies. It is the most common form of non-Hodgkin lymphoma among adults, with an annual incidence of 7–8 cases per 100,000 people per year in the US and UK. This cancer occurs primarily in older individuals, with a median age of diagnosis at ~70 years, although it can occur in young adults and, in rare cases, children. DLBCL can arise in virtually any part of the body and, depending on various factors, is often a very aggressive malignancy. The first sign of this illness is typically the observation of a rapidly growing mass or tissue infiltration that is sometimes associated with systemic B symptoms, e.g. fever, weight loss, and night sweats.
ABVD is a chemotherapy regimen used in the first-line treatment of Hodgkin lymphoma, replacing the older MOPP protocol. It consists of concurrent treatment with the chemotherapy drugs:
Richter's transformation (RT), also known as Richter's syndrome, is the conversion of chronic lymphocytic leukemia (CLL) or its variant, small lymphocytic lymphoma (SLL), into a new and more aggressively malignant disease. CLL is the circulation of malignant B lymphocytes with or without the infiltration of these cells into lymphatic or other tissues while SLL is the infiltration of these malignant B lymphocytes into lymphatic and/or other tissues with little or no circulation of these cells in the blood. CLL along with its SLL variant are grouped together in the term CLL/SLL.
Mantle cell lymphoma (MCL) is a type of non-Hodgkin's lymphoma, comprising about 6% of cases. It is named for the mantle zone of the lymph nodes where it develops. The term 'mantle cell lymphoma' was first adopted by Raffeld and Jaffe in 1991.
Chemoimmunotherapy is chemotherapy combined with immunotherapy. Chemotherapy uses different drugs to kill or slow the growth of cancer cells; immunotherapy uses treatments to stimulate or restore the ability of the immune system to fight cancer. A common chemoimmunotherapy regimen is CHOP combined with rituximab (CHOP-R) for B-cell non-Hodgkin lymphomas.

Aggressive lymphoma, also known as high-grade lymphoma, is a group of fast growing non-Hodgkin lymphoma.

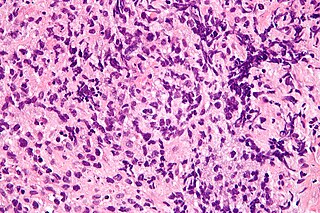
Follicular dendritic cell sarcoma (FDCS) is an extremely rare neoplasm. While the existence of FDC tumors was predicted by Lennert in 1978, the tumor wasn't fully recognized as its own cancer until 1986 after characterization by Monda et al. It accounts for only 0.4% of soft tissue sarcomas, but has significant recurrent and metastatic potential and is considered an intermediate grade malignancy. The major hurdle in treating FDCS has been misdiagnosis. It is a newly characterized cancer, and because of its similarities in presentation and markers to lymphoma, both Hodgkin and Non-Hodgkin subtypes, diagnosis of FDCS can be difficult. With recent advancements in cancer biology better diagnostic assays and chemotherapeutic agents have been made to more accurately diagnose and treat FDCS.
Brentuximab vedotin, sold under the brand name Adcetris, is an antibody-drug conjugate medication used to treat relapsed or refractory Hodgkin lymphoma (HL) and systemic anaplastic large cell lymphoma (ALCL), a type of T cell non-Hodgkin lymphoma. It selectively targets tumor cells expressing the CD30 antigen, a defining marker of Hodgkin lymphoma and ALCL. The drug is being jointly marketed by Millennium Pharmaceuticals outside the US and by Seagen in the US.
Primary mediastinal B-cell lymphoma, abbreviated PMBL, is a rare type of lymphoma that forms in the mediastinum and predominantly affects young adults.
VAMP regimen or VAMP chemotherapy is a four-drug combination chemotherapy regimen, used today in the treatment of Hodgkin lymphoma. It was one of the earliest combination chemotherapy regimens, originally developed as a treatment for childhood leukemia by a group of researchers at the National Cancer Institute led by Emil Frei and Emil Freireich. The first clinical trial of VAMP began in 1961. Because it was the first time that four chemotherapeutic agents were used at once, the trial was highly controversial at its time. Although new combination chemotherapy regimens have replaced the use of VAMP in the treatment of childhood leukemia, VAMP is considered an important precursor to modern treatments, confirming the effectiveness of combination chemotherapy and leading to the use of combination chemotherapy regimens to treat other types of cancer.

Plasmablastic lymphoma (PBL) is a type of large B-cell lymphoma recognized by the World Health Organization (WHO) in 2017 as belonging to a subgroup of lymphomas termed lymphoid neoplasms with plasmablastic differentiation. The other lymphoid neoplasms within this subgroup are: plasmablastic plasma cell lymphoma ; primary effusion lymphoma that is Kaposi's sarcoma-associated herpesvirus positive or Kaposi's sarcoma-associated Herpesvirus negative; anaplastic lymphoma kinase-positive large B-cell lymphoma; and human herpesvirus 8-positive diffuse large B-cell lymphoma, not otherwise specified. All of these lymphomas are malignancies of plasmablasts, i.e. B-cells that have differentiated into plasmablasts but because of their malignant nature: fail to differentiate further into mature plasma cells; proliferate excessively; and accumulate in and injure various tissues and organs.
R-HDAC, or R-HD-AraC ((R)ituximab plus (H)igh (D)ose (A)ra-(C)) is a chemotherapy regimen that is used, alternating with R-Maxi-CHOP, as part of so-called "Nordic protocol" of treating mantle cell lymphoma. It consists of monoclonal antibody rituximab and high-dose antimetabolite cytarabine.
EPOCH is an intensive chemotherapy regimen intended for treatment of aggressive non-Hodgkin's lymphoma.
CEPP is a chemotherapy regimen that is intended for treatment of aggressive non-Hodgkin lymphomas. It consists of cyclophosphamide, etoposide, procarbazine, and prednisone. Unlike CHOP, this chemotherapy regimen does not contain doxorubicin or any other anthracycline. Thus, it can be used in patients with severe cardiovascular diseases and contraindications for doxorubicin-containing regimens. This regimen also does not contain vincristine and can be used in patients with neuropathy.
FCM, or FMC in the context of chemotherapy is an acronym for a chemotherapy regimen that is used in the treatment of indolent B cell non-Hodgkin's lymphomas. In combination with Rituximab, this regimen is called R-FCM or R-FMC, or FCM-R, FMC-R.
"7+3" in the context of chemotherapy is an acronym for a chemotherapy regimen that is most often used today as first-line induction therapy in acute myelogenous leukemia, excluding the acute promyelocytic leukemia form, which is better treated with ATRA and/or arsenic trioxide and requires less chemotherapy.
Polatuzumab vedotin, sold under the brand name Polivy, is a CD79b-directed antibody-drug conjugate medication used for the treatment of diffuse large B-cell lymphoma (cancer). It was developed by the Genentech subsidiary of Roche.
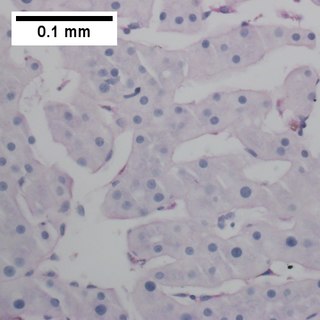
Primary testicular diffuse large B-cell lymphoma (PT-DLBCL), also termed testicular diffuse large B-cell lymphoma and diffuse large B-cell lymphoma of the testes, is a variant of the diffuse large B-cell lymphomas (DLBCL). DLBCL are a large and diverse group of B-cell malignancies with the great majority (-85%) being typed as diffuse large B-cell lymphoma, not otherwise specified. PT-DLBCL is a variant of DLBCL, NOS that involves one or, in uncommon cases, both testicles. Other variants and subtypes of DLBCL may involve the testes by spreading to them from their primary sites of origin in other tissues. PT-DLBCL differs from these other DLBCL in that it begins in the testes and then may spread to other sites.
