
Gastroenterology is the branch of medicine focused on the digestive system and its disorders. The digestive system consists of the gastrointestinal tract, sometimes referred to as the GI tract, which includes the esophagus, stomach, small intestine and large intestine as well as the accessory organs of digestion which include the pancreas, gallbladder, and liver. The digestive system functions to move material through the GI tract via peristalsis, break down that material via digestion, absorb nutrients for use throughout the body, and remove waste from the body via defecation. Physicians who specialize in the medical specialty of gastroenterology are called gastroenterologists or sometimes GI doctors. Some of the most common conditions managed by gastroenterologists include gastroesophageal reflux disease, gastrointestinal bleeding, irritable bowel syndrome, inflammatory bowel disease (IBD) which includes Crohn's disease and ulcerative colitis, peptic ulcer disease, gallbladder and biliary tract disease, hepatitis, pancreatitis, colitis, colon polyps and cancer, nutritional problems, and many more.

Crohn's disease is a type of inflammatory bowel disease (IBD) that may affect any segment of the gastrointestinal tract. Symptoms often include abdominal pain, diarrhea, fever, abdominal distension, and weight loss. Complications outside of the gastrointestinal tract may include anemia, skin rashes, arthritis, inflammation of the eye, and fatigue. The skin rashes may be due to infections as well as pyoderma gangrenosum or erythema nodosum. Bowel obstruction may occur as a complication of chronic inflammation, and those with the disease are at greater risk of colon cancer and small bowel cancer.

Ulcerative colitis (UC) is a type of inflammatory bowel disease (IBD). It is a long-term condition that results in inflammation and ulcers of the colon and rectum. The primary symptoms of active disease are abdominal pain and diarrhea mixed with blood (hematochezia). Weight loss, fever, and anemia may also occur. Often, symptoms come on slowly and can range from mild to severe. Symptoms typically occur intermittently with periods of no symptoms between flares. Complications may include abnormal dilation of the colon (megacolon), inflammation of the eye, joints, or liver, and colon cancer.

The gastrointestinal tract is the tract or passageway of the digestive system that leads from the mouth to the anus. The GI tract contains all the major organs of the digestive system, in humans and other animals, including the esophagus, stomach, and intestines. Food taken in through the mouth is digested to extract nutrients and absorb energy, and the waste expelled at the anus as faeces. Gastrointestinal is an adjective meaning of or pertaining to the stomach and intestines.

An endoscopy is a procedure used in medicine to look inside the body. The endoscopy procedure uses an endoscope to examine the interior of a hollow organ or cavity of the body. Unlike many other medical imaging techniques, endoscopes are inserted directly into the organ.
An endoscope is an inspection instrument composed of image sensor, optical lens, light source and mechanical device, which is used to look deep into the body by way of openings such as the mouth or anus. A typical endoscope applies several modern technologies including optics, ergonomics, precision mechanics, electronics, and software engineering. With an endoscope, it is possible to observe lesions that cannot be detected by X-ray, making it useful in medical diagnosis. Endoscopes use tubes which are only a few millimeters thick to transfer illumination in one direction and high-resolution images in real time in the other direction, resulting in minimally invasive surgeries. It is used to examine the internal organs like the throat or esophagus. Specialized instruments are named after their target organ. Examples include the cystoscope (bladder), nephroscope (kidney), bronchoscope (bronchus), arthroscope (joints) and colonoscope (colon), and laparoscope. They can be used to examine visually and diagnose, or assist in surgery such as an arthroscopy.

Enteritis is inflammation of the small intestine. It is most commonly caused by food or drink contaminated with pathogenic microbes, such as Serratia, but may have other causes such as NSAIDs, radiation therapy as well as autoimmune conditions like Crohn's disease and celiac disease. Symptoms include abdominal pain, cramping, diarrhea, dehydration, and fever. Related diseases of the gastrointestinal system involve inflammation of the stomach and large intestine.

An upper gastrointestinal series, also called a barium swallow, barium study, or barium meal, is a series of radiographs used to examine the gastrointestinal tract for abnormalities. A contrast medium, usually a radiocontrast agent such as barium sulfate mixed with water, is ingested or instilled into the gastrointestinal tract, and X-rays are used to create radiographs of the regions of interest. The barium enhances the visibility of the relevant parts of the gastrointestinal tract by coating the inside wall of the tract and appearing white on the film. This in combination with other plain radiographs allows for the imaging of parts of the upper gastrointestinal tract such as the pharynx, larynx, esophagus, stomach, and small intestine such that the inside wall lining, size, shape, contour, and patency are visible to the examiner. With fluoroscopy, it is also possible to visualize the functional movement of examined organs such as swallowing, peristalsis, or sphincter closure. Depending on the organs to be examined, barium radiographs can be classified into "barium swallow", "barium meal", "barium follow-through", and "enteroclysis". To further enhance the quality of images, air or gas is sometimes introduced into the gastrointestinal tract in addition to barium, and this procedure is called double-contrast imaging. In this case the gas is referred to as the negative contrast medium. Traditionally the images produced with barium contrast are made with plain-film radiography, but computed tomography is also used in combination with barium contrast, in which case the procedure is called "CT enterography".

In medicine (gastroenterology), angiodysplasia is a small vascular malformation of the gut. It is a common cause of otherwise unexplained gastrointestinal bleeding and anemia. Lesions are often multiple, and frequently involve the cecum or ascending colon, although they can occur at other places. Treatment may be with colonoscopic interventions, angiography and embolization, medication, or occasionally surgery.

Esophagogastroduodenoscopy (EGD) or oesophagogastroduodenoscopy (OGD), also called by various other names, is a diagnostic endoscopic procedure that visualizes the upper part of the gastrointestinal tract down to the duodenum. It is considered a minimally invasive procedure since it does not require an incision into one of the major body cavities and does not require any significant recovery after the procedure. However, a sore throat is common.
Gastrointestinal bleeding, also called gastrointestinal hemorrhage (GIB), is all forms of bleeding in the gastrointestinal tract, from the mouth to the rectum. When there is significant blood loss over a short time, symptoms may include vomiting red blood, vomiting black blood, bloody stool, or black stool. Small amounts of bleeding over a long time may cause iron-deficiency anemia resulting in feeling tired or heart-related chest pain. Other symptoms may include abdominal pain, shortness of breath, pale skin, or passing out. Sometimes in those with small amounts of bleeding no symptoms may be present.

Gastrointestinal diseases refer to diseases involving the gastrointestinal tract, namely the esophagus, stomach, small intestine, large intestine and rectum, and the accessory organs of digestion, the liver, gallbladder, and pancreas.
Blood in stool or rectal bleeding looks different depending on how early it enters the digestive tract—and thus how much digestive action it has been exposed to—and how much there is. The term can refer either to melena, with a black appearance, typically originating from upper gastrointestinal bleeding; or to hematochezia, with a red color, typically originating from lower gastrointestinal bleeding. Evaluation of the blood found in stool depends on its characteristics, in terms of color, quantity and other features, which can point to its source, however, more serious conditions can present with a mixed picture, or with the form of bleeding that is found in another section of the tract. The term "blood in stool" is usually only used to describe visible blood, and not fecal occult blood, which is found only after physical examination and chemical laboratory testing.
Enteroscopy is the procedure of using an endoscope for the direct visualization of the small bowel. Etymologically, the word could potentially refer to any bowel endoscopy, but idiomatically it is conventionally restricted to small bowel endoscopy, in distinction from colonoscopy, which is large bowel endoscopy. Various types of enteroscopy exist, as follows:

Double-balloon enteroscopy, also known as push-and-pull enteroscopy, is an endoscopic technique for visualization of the small bowel. It was developed by Hironori Yamamoto in 2001. It is novel in the field of diagnostic gastroenterology as it is the first endoscopic technique that allows for the entire gastrointestinal tract to be visualized in real time.

SeHCAT is a drug used in a clinical test to diagnose bile acid malabsorption.

Given Imaging is an Israeli medical technology company that manufactures and markets diagnostic products for the visualization and detection of disorders of the gastrointestinal tract. Until March 2014, it was dual-listed on both the NASDAQ and the Tel Aviv Stock Exchange, where it was a component of the TA-100 Index and the TA BlueTech Index. In March 2014 it was acquired by Covidien and became a private company. In 2015 Covidien was purchased by Medtronic.
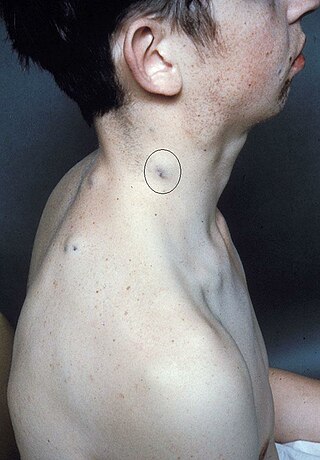
Blue rubber bleb nevus syndrome is a rare disorder that consists mainly of abnormal blood vessels affecting the skin or internal organs – usually the gastrointestinal tract. The disease is characterized by the presence of fluid-filled blisters (blebs) as visible, circumscribed, chronic lesions (nevi).
Blair S. Lewis, M.D., F.A.C.P., F.A.C.G., is an American board-certified gastroenterologist and Clinical Professor of Medicine at the Mount Sinai School of Medicine. Lewis is a specialist in the field of gastrointestinal endoscopy and was the primary investigator for the first clinical trial of capsule endoscopy for the small intestine and also the first clinical trial of capsule endoscopy for the colon.
Computed tomography enterography is a medical imaging technique which uses computed tomography scanner and contrast media to examine the small bowel. It was first introduced by Raptopoulos et al. in 1997. CT Enterography can be used to assess a variety of problems involving the small bowel, however it is mainly used to diagnose and assess severity of Crohn's disease.



