Related Research Articles
An eating disorder is a mental disorder defined by abnormal eating behaviors that negatively affect a person's physical or mental health. Types of eating disorders include binge eating disorder, where the patient eats a large amount in a short period of time; anorexia nervosa, where the person has an intense fear of gaining weight and restricts food or overexercises to manage this fear; bulimia nervosa, where individuals eat a large quantity (binging) then try to rid themselves of the food (purging); pica, where the patient eats non-food items; rumination syndrome, where the patient regurgitates undigested or minimally digested food; avoidant/restrictive food intake disorder (ARFID), where people have a reduced or selective food intake due to some psychological reasons; and a group of other specified feeding or eating disorders. Anxiety disorders, depression and substance abuse are common among people with eating disorders. These disorders do not include obesity. People often experience comorbidity between an eating disorder and OCD. It is estimated 20–60% of patients with an ED have a history of OCD.

Bulimia nervosa, also known as simply bulimia, is an eating disorder characterized by binge eating followed by purging or fasting, and excessive concern with body shape and weight. This activity aims to expel the body of calories eaten from the binging phase of the process. Binge eating refers to eating a large amount of food in a short amount of time. Purging refers to the attempts to get rid of the food consumed. This may be done by vomiting or taking laxatives.
Pica is the eating or craving of things that are not food. It is classified as an eating disorder but can also be the result of an existing mental disorder. The ingested or craved substance may be biological, natural or manmade. The term was drawn directly from the medieval Latin word for magpie, a bird subject to much folklore regarding its opportunistic feeding behaviors.

Dysphagia is difficulty in swallowing. Although classified under "symptoms and signs" in ICD-10, in some contexts it is classified as a condition in its own right.
Appetite is the desire to eat food items, usually due to hunger. Appealing foods can stimulate appetite even when hunger is absent, although appetite can be greatly reduced by satiety. Appetite exists in all higher life-forms, and serves to regulate adequate energy intake to maintain metabolic needs. It is regulated by a close interplay between the digestive tract, adipose tissue and the brain. Appetite has a relationship with every individual's behavior. Appetitive behaviour also known as approach behaviour, and consummatory behaviour, are the only processes that involve energy intake, whereas all other behaviours affect the release of energy. When stressed, appetite levels may increase and result in an increase of food intake. Decreased desire to eat is termed anorexia, while polyphagia is increased eating. Dysregulation of appetite contributes to anorexia nervosa, bulimia nervosa, cachexia, overeating, and binge eating disorder.
Emetophobia is a phobia that causes overwhelming, intense anxiety pertaining to vomit. This specific phobia can also include subcategories of what causes the anxiety, including a fear of vomiting or seeing others vomit. Emetephobes might also avoid the mentions of "barfing", vomiting, "throwing up", or "puking."
Neophobia is the fear of anything new, especially a persistent and abnormal fear. In its milder form, it can manifest as the unwillingness to try new things or break from routine. In the context of children the term is generally used to indicate a tendency to reject unknown or novel foods. Food neophobia, as it may be referred to, is an important concern in pediatric psychology.

A feeding tube is a medical device used to provide nutrition to people who cannot obtain nutrition by mouth, are unable to swallow safely, or need nutritional supplementation. The state of being fed by a feeding tube is called gavage, enteral feeding or tube feeding. Placement may be temporary for the treatment of acute conditions or lifelong in the case of chronic disabilities. A variety of feeding tubes are used in medical practice. They are usually made of polyurethane or silicone. The diameter of a feeding tube is measured in French units. They are classified by the site of insertion and intended use.

Failure to thrive (FTT), also known as weight faltering or faltering growth, indicates insufficient weight gain or absence of appropriate physical growth in children. FTT is usually defined in terms of weight, and can be evaluated either by a low weight for the child's age, or by a low rate of increase in the weight.

Tongue thrust is a pseudo-pathological name of what is either considered a normal adaptive lip seal mechanism, whereby normal nasal breathing or normal swallowing can occur, or seen as an oral myofunctional disorder - a tongue muscle pattern that is perceived as clinically abnormal and in which the tongue protrudes anteriorly to seal otherwise incompetent lips.
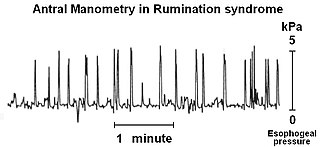
Rumination syndrome, or merycism, is a chronic motility disorder characterized by effortless regurgitation of most meals following consumption, due to the involuntary contraction of the muscles around the abdomen. There is no retching, nausea, heartburn, odour, or abdominal pain associated with the regurgitation, as there is with typical vomiting, and the regurgitated food is undigested. The disorder has been historically documented as affecting only infants, young children, and people with cognitive disabilities . It is increasingly being diagnosed in a greater number of otherwise healthy adolescents and adults, though there is a lack of awareness of the condition by doctors, patients and the general public.
Oropharyngeal dysphagia arises from abnormalities of muscles, nerves or structures of the oral cavity, pharynx, and upper esophageal sphincter.
Pseudodysphagia, in its severe form, is the irrational fear of swallowing or, in its minor form, of choking. The symptoms are psychosomatic, so while the sensation of difficult swallowing feels authentic to the individual, it is not based on a real physical symptom. It is important that dysphagia be ruled out before a diagnosis of pseudodysphagia is made.
Baby-led weaning is an approach to adding complementary foods to a baby's diet of breast milk or formula. BLW facilitates oral motor development and strongly focuses on the family meal, while maintaining eating as a positive, interactive experience. Baby-led weaning allows babies to control their solid food consumption by "self-feeding" from the start of their experience with food. The term weaning does not imply giving up breast milk or formula, but simply indicates the introduction of foods other than breast milk or formula.

Aphagia is the inability or refusal to swallow. The word is derived from the Ancient Greek prefix α, meaning "not" or "without," and the suffix φαγία, derived from the verb φαγεῖν, meaning "to eat." It is related to dysphagia which is difficulty swallowing, and odynophagia, painful swallowing. Aphagia may be temporary or long term, depending on the affected organ. It is an extreme, life-threatening case of dysphagia. Depending on the cause, untreated dysphagia may develop into aphagia.
Avoidant/restrictive food intake disorder (ARFID) is a feeding or eating disorder in which people avoid eating or eat only a very narrow range of foods. This can be due to the sensory characteristics of food, such as its appearance, smell, texture, or taste, and/or due to fear of negative consequences such as choking or vomiting; and/or having little interest in eating or food.
Gastroparesis, also called delayed gastric emptying, is a medical disorder consisting of weak muscular contractions (peristalsis) of the stomach, resulting in food and liquid remaining in the stomach for a prolonged period of time. Stomach contents thus exit more slowly into the duodenum of the digestive tract. This can result in irregular absorption of nutrients, inadequate nutrition, and poor glycemic control.
Mental disorders diagnosed in childhood can be neurodevelopmental, emotional, or behavioral disorders. These disorders negatively impact the mental and social wellbeing of a child, and children with these disorders require support from their families and schools. Childhood mental disorders often persist into adulthood. These disorders are usually first diagnosed in infancy, childhood, or adolescence, as laid out in the DSM-5 and in the ICD-11.

Anorexia nervosa (AN), often referred to simply as anorexia, is an eating disorder characterized by low weight, food restriction, body image disturbance, fear of gaining weight, and an overpowering desire to be thin.
The Graz tube weaning model is a method that supports parents, caregivers and professionals to help and empower medically fragile children with early and post-traumatic eating behavior disorders, particularly tube dependency.
References
- 1 2 3 "Feeding disorder of infancy or early childhood". Encyclopedia of Mental Disorders. Advameg, Inc. Retrieved 26 February 2011.
- ↑ Sexson, Sandra B. (2005). Child and adolescent psychiatry . Wiley-Blackwell. pp. 399. ISBN 1-4051-1768-0.
- 1 2 "Feeding Disorders". Kennedy Krieger Institute. Archived from the original on 26 July 2011. Retrieved 8 July 2011.
- ↑ "Feeding Disorders". Feeding Clinic of Santa Monica. Archived from the original on 19 September 2018. Retrieved 8 July 2013.
- ↑ "Feeding Disorders". Kennedy Krieger Institute. 2012. Retrieved 16 December 2013.
- ↑ "Feeding Disorders". Archived from the original on 27 May 2010. Retrieved 18 July 2011.
- ↑ "Feeding Disorders and swallowing disorders" . Retrieved 18 July 2011.
- ↑ Patel, M. R.; Piazza, C. C.; Martinez, C. J.; Volkert, V. M.; Christine, M. S. (2002). "An evaluation of two differential reinforcement procedures with escape extinction to treat food refusal". Journal of Applied Behavior Analysis. 35 (4): 363–374. doi:10.1901/jaba.2002.35-363. PMC 1284399 . PMID 12555908.
- ↑ "5 Things to Know About Feeding Therapy". Harrison Speech Pathology. 2019-07-04. Retrieved 2019-08-14.
- ↑ Andrea Barkoukis; Natalie Staats Reiss; Mark Dombeck. "Feeding Disorder of Early Childhood" . Retrieved 26 June 2011.
- ↑ Bernard-Bonnin, AC (2006). "Feeding problems of infants and toddlers". Canadian Family Physician. 52 (10): 1247–1251. PMC 1783606 . PMID 17279184.
- ↑ Kay, Jerald (2006). Essentials of Psychiatry. West Sussex: John Wiley & Sons Ltd. p. 1078. ISBN 0-470-01854-2.