
Otorhinolaryngology is a surgical subspecialty within medicine that deals with the surgical and medical management of conditions of the head and neck. Doctors who specialize in this area are called otorhinolaryngologists, otolaryngologists, head and neck surgeons, or ENT surgeons or physicians. Patients seek treatment from an otorhinolaryngologist for diseases of the ear, nose, throat, base of the skull, head, and neck. These commonly include functional diseases that affect the senses and activities of eating, drinking, speaking, breathing, swallowing, and hearing. In addition, ENT surgery encompasses the surgical management of cancers and benign tumors and reconstruction of the head and neck as well as plastic surgery of the face, scalp, and neck.
Sinusitis, also known as rhinosinusitis, is an inflammation of the mucous membranes that line the sinuses resulting in symptoms that may include thick nasal mucus, a plugged nose, and facial pain.

Nasal polyps (NP) are noncancerous growths within the nose or sinuses. Symptoms include trouble breathing through the nose, loss of smell, decreased taste, post nasal drip, and a runny nose. The growths are sac-like, movable, and nontender, though face pain may occasionally occur. They typically occur in both nostrils in those who are affected. Complications may include sinusitis and broadening of the nose.

Nasal irrigation is a personal hygiene practice in which the nasal cavity is washed to flush out mucus and debris from the nose and sinuses, in order to enhance nasal breathing. Nasal irrigation can also refer to the use of saline nasal spray or nebulizers to moisten the mucous membranes.
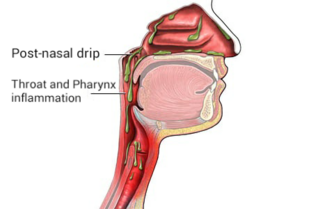
Post-nasal drip (PND), also known as upper airway cough syndrome (UACS), occurs when excessive mucus is produced by the nasal mucosa. The excess mucus accumulates in the back of the nose, and eventually in the throat once it drips down the back of the throat. It can be caused by rhinitis, sinusitis, gastroesophageal reflux disease (GERD), or by a disorder of swallowing. Other causes can be allergy, cold, flu, and side effects from medications.
Balloon sinuplasty is a procedure that ear, nose and throat surgeons may use for the treatment of blocked sinuses. Patients diagnosed with sinusitis but not responding to medications may be candidates for sinus surgery. Balloon technology was initially cleared by the U.S. Food and Drug Administration in 2005 and is an endoscopic, catheter-based system for chronic sinusitis. It uses a balloon over a wire catheter to dilate sinus passageways. The balloon is inflated with the goal of dilating the sinus openings, widening the walls of the sinus passageway and restoring normal drainage.
Chronic atrophic rhinitis, or simply atrophic rhinitis, is a chronic inflammation of the nose characterised by atrophy of nasal mucosa, including the glands, turbinate bones and the nerve elements supplying the nose. Chronic atrophic rhinitis may be primary and secondary. Special forms of chronic atrophic rhinitis are rhinitis sicca anterior and ozaena. It can also be described as the empty nose syndrome.
Rhinosinusitis is a simultaneous infection of the nasal mucosa (rhinitis) and an infection of the mucosa of the paranasal sinuses (sinusitis). A distinction is made between acute rhinosinusitis and chronic rhinosinusitis.

An inverted papilloma, also known as Ringertz tumour, is a type of tumor in which surface epithelial cells grow downward into the underlying supportive tissue. It may occur in the nose and/or sinuses or in the urinary tract. When it occurs in the nose or sinuses, it may cause symptoms similar to those caused by sinusitis, such as nasal congestion. When it occurs in the urinary tract, it may cause blood in the urine.
Endoscopic ear surgery (EES) is a minimally invasive alternative to traditional ear surgery and is defined as the use of the rigid endoscope, as opposed to a surgical microscope, to visualize the middle and inner ear during otologic surgery. During endoscopic ear surgery the surgeon holds the endoscope in one hand while working in the ear with the other. To allow this kind of single-handed surgery, different surgical instruments have to be used. Endoscopic visualization has improved due to high-definition video imaging and wide-field endoscopy, and being less invasive, EES is gaining importance as an adjunct to microscopic ear surgery.
Antral lavage is a largely obsolete surgical procedure in which a cannula is inserted into the maxillary sinus via the inferior meatus to allow irrigation and drainage of the sinus. It is also called proof puncture, as the presence of an infection can be proven during the procedure. Upon presence of infection, it can be considered as therapeutic puncture. Often, multiple repeated lavages are subsequently required to allow for full washout of infection.
Caldwell-Luc surgery, Caldwell-Luc operation, also known as Caldwell-Luc antrostomy, and Radical antrostomy, is an operation to remove irreversibly damaged mucosa of the maxillary sinus. It is done when maxillary sinusitis is not cured by medication or other non-invasive technique. The approach is mainly from the anterior wall of the maxilla bone. It was introduced by George Caldwell (1893)and Henry Luc (1897). The maxillary sinus is entered from two separate openings, one in the canine fossa to gain access to the antrum and other in the naso antral wall for drainage.
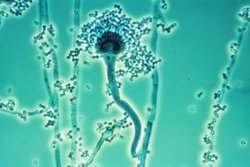
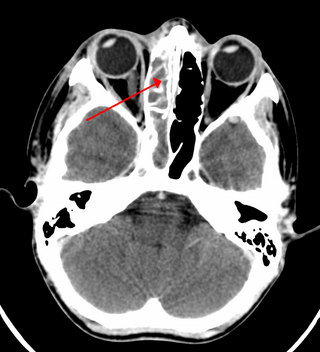
Fungal sinusitis or fungal rhinosinusitis is the inflammation of the lining mucosa of the paranasal sinuses due to a fungal infection. It occurs in people with reduced immunity. The maxillary sinus is the most commonly involved. Fungi responsible for fungal sinusitis are Aspergillus fumigatus (90%), Aspergillus flavus, and Aspergillus niger. Fungal sinusitis occurs most commonly in middle-aged populations. Diabetes mellitus is the most common risk factor involved.
Eustachian tube dysfunction (ETD) is a disorder where pressure abnormalities in the middle ear result in symptoms.
Muaaz Tarabichi is a Syrian otolaryngologist, lecturer, researcher, and author. He is recognized around the world as the father of endoscopic ear surgery. He is the co-founder of Tarabichi Stammberger Ear and Sinus Institute. He was elected as the chairman of the International Advisory Board of the American Academy of Otolaryngology–Head and Neck Surgery.

Heinz Stammberger (1946-2018) was a German-Austrian teacher, and researcher in the field of sinus surgery and otolaryngology. He was an Emeritus Professor and Head of the Department of General ORL, H&NS of the Medical University of Graz.
Nasal surgery is a medical procedure designed to treat various conditions that cause nasal blockages in the upper respiratory tract, for example nasal polyps, inferior turbinate hypertrophy, and chronic rhinosinusitis. It encompasses several types of techniques, including rhinoplasty, septoplasty, sinus surgery, and turbinoplasty, each with its respective postoperative treatments. Furthermore, nasal surgery is also conducted for cosmetic purposes. While there are potential risks and complications associated, the advancement of medical instruments and enhanced surgical skills have helped mitigate them.

Odontogenic sinusitis is a type of sinusitis, specifically caused by dental infections or procedures. Comprising approximately 10-12% of all chronic sinusitis cases, this condition primarily affects the maxillary sinus, which is in close proximity to the upper teeth.

Dame Valerie Joan Lund is a British surgeon and emeritus Professor in Rhinology at University College London. Lund has worked on endoscopic endonasal surgery and studies sinonasal conditions She was elevated from CBE to DBE in the 2024 New Year Honours.
David William Kennedy is an American academician, surgeon, and otolaryngologist. He is currently serving as an emeritus professor at the University of Pennsylvania.


