
Sleep is a state of reduced mental and physical activity in which consciousness is altered and sensory activity is inhibited to a certain extent. During sleep, there is a decrease in muscle activity, and interactions with the surrounding environment. While sleep differs from wakefulness in terms of the ability to react to stimuli, it still involves active brain patterns, making it more reactive than a coma or disorders of consciousness.

A sleep disorder, or somnipathy, is a medical disorder of an individual's sleep patterns. Some sleep disorders are severe enough to interfere with normal physical, mental, social and emotional functioning. Polysomnography and actigraphy are tests commonly ordered for diagnosing sleep disorders.
Rapid eye movement sleep is a unique phase of sleep in humans, mammals and birds, characterized by random rapid movement of the eyes, accompanied by low muscle tone throughout the body, and the propensity of the sleeper to dream vividly.

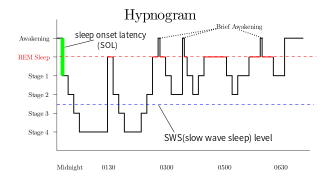
The sleep cycle is an oscillation between the slow-wave and REM (paradoxical) phases of sleep. It is sometimes called the ultradian sleep cycle, sleep–dream cycle, or REM-NREM cycle, to distinguish it from the circadian alternation between sleep and wakefulness. In humans, this cycle takes 70 to 110 minutes.

{

Nightmare disorder is a sleep disorder characterized by repeated intense nightmares that most often center on threats to physical safety and security. The nightmares usually occur during the REM stage of sleep, and the person who experiences the nightmares typically remembers them well upon waking. More specifically, nightmare disorder is a type of parasomnia, a subset of sleep disorders categorized by abnormal movement or behavior or verbal actions during sleep or shortly before or after. Other parasomnias include sleepwalking, sleep terrors, bedwetting, and sleep paralysis.
Non-rapid eye movement sleep (NREM), also known as quiescent sleep, is, collectively, sleep stages 1–3, previously known as stages 1–4. Rapid eye movement sleep (REM) is not included. There are distinct electroencephalographic and other characteristics seen in each stage. Unlike REM sleep, there is usually little or no eye movement during these stages. Dreaming occurs during both sleep states, and muscles are not paralyzed as in REM sleep. People who do not go through the sleeping stages properly get stuck in NREM sleep, and because muscles are not paralyzed a person may be able to sleepwalk. According to studies, the mental activity that takes place during NREM sleep is believed to be thought-like, whereas REM sleep includes hallucinatory and bizarre content. NREM sleep is characteristic of dreamer-initiated friendliness, compared to REM sleep where it's more aggressive, implying that NREM is in charge of simulating friendly interactions. The mental activity that occurs in NREM and REM sleep is a result of two different mind generators, which also explains the difference in mental activity. In addition, there is a parasympathetic dominance during NREM. The reported differences between the REM and NREM activity are believed to arise from differences in the memory stages that occur during the two types of sleep.
Sexsomnia, also known as sleep sex, is a distinct form of parasomnia, or an abnormal activity that occurs while an individual is asleep. Sexsomnia is characterized by an individual engaging in sexual acts while in non-rapid eye movement (NREM) sleep. Sexual behaviors that result from sexsomnia are not to be mistaken with normal nocturnal sexual behaviors, which do not occur during NREM sleep. Sexual behaviors that are viewed as normal during sleep and are accompanied by extensive research and documentation include nocturnal emissions, nocturnal erections, and sleep orgasms.
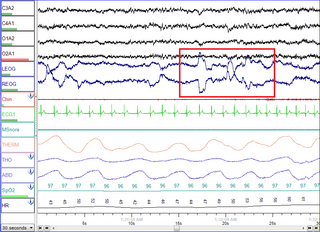
Polysomnography (PSG), a type of sleep study, is a multi-parameter study of sleep and a diagnostic tool in sleep medicine. The test result is called a polysomnogram, also abbreviated PSG. The name is derived from Greek and Latin roots: the Greek πολύς, the Latin somnus ("sleep"), and the Greek γράφειν.
The cyclic alternating pattern is a pattern of two, long-lasting alternate electroencephalogram (EEG) patterns that occur in sleep, as described by Terzano, et al., in 1985. It is a pattern of spontaneous cortical activity, which is ongoing and in the absence of sensory stimulation. It is the reorganization of the sleeping brain challenged by the modification of environmental conditions and it is characterized by periodic abnormal electrocortical activity that recurs with a frequency of up to one minute. It is considered "the EEG marker of unstable sleep". CAP does not occur during REM. In Lennox-Gastaut syndrome, CAP modulates the occurrence of clinical seizures and generalized epileptic discharges by means of a gate-control mechanism.

A K-complex is a waveform that may be seen on an electroencephalogram (EEG). It occurs during stage 2 NREM sleep. It is the "largest event in healthy human EEG". They are more frequent in the first sleep cycles.
Sleep spindles are bursts of neural oscillatory activity that are generated by interplay of the thalamic reticular nucleus (TRN) and other thalamic nuclei during stage 2 NREM sleep in a frequency range of ~11 to 16 Hz with a duration of 0.5 seconds or greater. After generation as an interaction of the TRN neurons and thalamocortical cells, spindles are sustained and relayed to the cortex by thalamo-thalamic and thalamo-cortical feedback loops regulated by both GABAergic and NMDA-receptor mediated glutamatergic neurotransmission. Sleep spindles have been reported for all tested mammalian species. Considering animals in which sleep-spindles were studied extensively, they appear to have a conserved main frequency of roughly 9–16 Hz. Only in humans, rats and dogs is a difference in the intrinsic frequency of frontal and posterior spindles confirmed, however.

Slow-wave sleep (SWS), often referred to as deep sleep, consists of stage three of non-rapid eye movement sleep. It usually lasts between 70 and 90 minutes and takes place during the first hours of the night. Initially, SWS consisted of both Stage 3, which has 20–50 percent delta wave activity, and Stage 4, which has more than 50 percent delta wave activity.
Parasomnias are a category of sleep disorders that involve abnormal movements, behaviors, emotions, perceptions, and dreams that occur while falling asleep, sleeping, between sleep stages, or during arousal from sleep. Parasomnias are dissociated sleep states which are partial arousals during the transitions between wakefulness, NREM sleep, and REM sleep, and their combinations.
Allan Rechtschaffen was a noted pioneer in the field of sleep research whose work includes some of the first laboratory studies of insomnia, narcolepsy, sleep apnea, and napping. He received his PhD from Northwestern University in 1956.

Sleep in animals refers to a behavioral and physiological state characterized by altered consciousness, reduced responsiveness to external stimuli, and homeostatic regulation observed in various animals. Sleep has been observed in mammals, birds, reptiles, amphibians, and some fish, and, in some form, in insects and even in simpler animals such as nematodes. The internal circadian clock promotes sleep at night for diurnal organisms and in the day for nocturnal organisms. Sleep patterns vary widely among species. It appears to be a requirement for all mammals and most other animals.
Sleep onset is the transition from wakefulness into sleep. Sleep onset usually transmits into non-rapid eye movement sleep but under certain circumstances it is possible to transit from wakefulness directly into rapid eye movement sleep.

The relationship between sleep and memory has been studied since at least the early 19th century. Memory, the cognitive process of storing and retrieving past experiences, learning and recognition, is a product of brain plasticity, the structural changes within synapses that create associations between stimuli. Stimuli are encoded within milliseconds; however, the long-term maintenance of memories can take additional minutes, days, or even years to fully consolidate and become a stable memory that is accessible. Therefore, the formation of a specific memory occurs rapidly, but the evolution of a memory is often an ongoing process.

The neuroscience of sleep is the study of the neuroscientific and physiological basis of the nature of sleep and its functions. Traditionally, sleep has been studied as part of psychology and medicine. The study of sleep from a neuroscience perspective grew to prominence with advances in technology and the proliferation of neuroscience research from the second half of the twentieth century.
An electrogram (EGM) is a recording of electrical activity of organs such as the brain and heart, measured by monitoring changes in electric potential.

