Related Research Articles

Hearing loss is a partial or total inability to hear. Hearing loss may be present at birth or acquired at any time afterwards. Hearing loss may occur in one or both ears. In children, hearing problems can affect the ability to acquire spoken language, and in adults it can create difficulties with social interaction and at work. Hearing loss can be temporary or permanent. Hearing loss related to age usually affects both ears and is due to cochlear hair cell loss. In some people, particularly older people, hearing loss can result in loneliness.
The absolute threshold of hearing (ATH), also known as the absolute hearing threshold or auditory threshold, is the minimum sound level of a pure tone that an average human ear with normal hearing can hear with no other sound present. The absolute threshold relates to the sound that can just be heard by the organism. The absolute threshold is not a discrete point and is therefore classed as the point at which a sound elicits a response a specified percentage of the time.

In acoustics, loudness is the subjective perception of sound pressure. More formally, it is defined as the "attribute of auditory sensation in terms of which sounds can be ordered on a scale extending from quiet to loud". The relation of physical attributes of sound to perceived loudness consists of physical, physiological and psychological components. The study of apparent loudness is included in the topic of psychoacoustics and employs methods of psychophysics.
Auditory neuropathy (AN) is a hearing disorder in which the outer hair cells of the cochlea are present and functional, but sound information is not transmitted sufficiently by the auditory nerve to the brain. The cause may be several dysfunctions of the inner hair cells of the cochlea or spiral ganglion neuron levels. Hearing loss with AN can range from normal hearing sensitivity to profound hearing loss.
Unilateral hearing loss (UHL) is a type of hearing impairment where there is normal hearing in one ear and impaired hearing in the other ear.
Presbycusis, or age-related hearing loss, is the cumulative effect of aging on hearing. It is a progressive and irreversible bilateral symmetrical age-related sensorineural hearing loss resulting from degeneration of the cochlea or associated structures of the inner ear or auditory nerves. The hearing loss is most marked at higher frequencies. Hearing loss that accumulates with age but is caused by factors other than normal aging is not presbycusis, although differentiating the individual effects of distinct causes of hearing loss can be difficult.

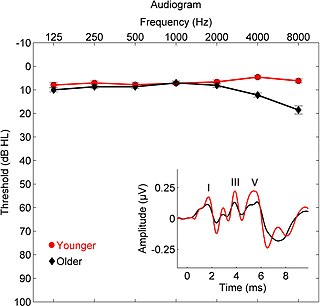
An audiogram is a graph that shows the audible threshold for standardized frequencies as measured by an audiometer. The Y axis represents intensity measured in decibels (dB) and the X axis represents frequency measured in hertz (Hz). The threshold of hearing is plotted relative to a standardised curve that represents 'normal' hearing, in dB(HL). They are not the same as equal-loudness contours, which are a set of curves representing equal loudness at different levels, as well as at the threshold of hearing, in absolute terms measured in dB SPL.
The auditory brainstem response (ABR), also called brainstem evoked response audiometry (BERA) or brainstem auditory evoked potentials (BAEPs) or brainstem auditory evoked responses (BAERs) is an auditory evoked potential extracted from ongoing electrical activity in the brain and recorded via electrodes placed on the scalp. The measured recording is a series of six to seven vertex positive waves of which I through V are evaluated. These waves, labeled with Roman numerals in Jewett and Williston convention, occur in the first 10 milliseconds after onset of an auditory stimulus. The ABR is considered an exogenous response because it is dependent upon external factors.
Binaural fusion or binaural integration is a cognitive process that involves the combination of different auditory information presented binaurally, or to each ear. In humans, this process is essential in understanding speech as one ear may pick up more information about the speech stimuli than the other.

Pure-tone audiometry is the main hearing test used to identify hearing threshold levels of an individual, enabling determination of the degree, type and configuration of a hearing loss and thus providing a basis for diagnosis and management. Pure-tone audiometry is a subjective, behavioural measurement of a hearing threshold, as it relies on patient responses to pure tone stimuli. Therefore, pure-tone audiometry is only used on adults and children old enough to cooperate with the test procedure. As with most clinical tests, standardized calibration of the test environment, the equipment and the stimuli is needed before testing proceeds. Pure-tone audiometry only measures audibility thresholds, rather than other aspects of hearing such as sound localization and speech recognition. However, there are benefits to using pure-tone audiometry over other forms of hearing test, such as click auditory brainstem response (ABR). Pure-tone audiometry provides ear specific thresholds, and uses frequency specific pure tones to give place specific responses, so that the configuration of a hearing loss can be identified. As pure-tone audiometry uses both air and bone conduction audiometry, the type of loss can also be identified via the air-bone gap. Although pure-tone audiometry has many clinical benefits, it is not perfect at identifying all losses, such as ‘dead regions’ of the cochlea and neuropathies such as auditory processing disorder (APD). This raises the question of whether or not audiograms accurately predict someone's perceived degree of disability.
Auditory processing disorder (APD), rarely known as King-Kopetzky syndrome or auditory disability with normal hearing (ADN), is a neurodevelopmental disorder affecting the way the brain processes sounds. Individuals with APD usually have normal structure and function of the ear, but cannot process the information they hear in the same way as others do, which leads to difficulties in recognizing and interpreting sounds, especially the sounds composing speech. It is thought that these difficulties arise from dysfunction in the central nervous system. This is, in part, essentially a failure of the cocktail party effect found in most people.
Spatial hearing loss refers to a form of deafness that is an inability to use spatial cues about where a sound originates from in space. Poor sound localization in turn affects the ability to understand speech in the presence of background noise.
Amblyaudia is a term coined by Dr. Deborah Moncrieff to characterize a specific pattern of performance from dichotic listening tests. Dichotic listening tests are widely used to assess individuals for binaural integration, a type of auditory processing skill. During the tests, individuals are asked to identify different words presented simultaneously to the two ears. Normal listeners can identify the words fairly well and show a small difference between the two ears with one ear slightly dominant over the other. For the majority of listeners, this small difference is referred to as a "right-ear advantage" because their right ear performs slightly better than their left ear. But some normal individuals produce a "left-ear advantage" during dichotic tests and others perform at equal levels in the two ears. Amblyaudia is diagnosed when the scores from the two ears are significantly different with the individual's dominant ear score much higher than the score in the non-dominant ear Researchers interested in understanding the neurophysiological underpinnings of amblyaudia consider it to be a brain based hearing disorder that may be inherited or that may result from auditory deprivation during critical periods of brain development. Individuals with amblyaudia have normal hearing sensitivity but have difficulty hearing in noisy environments like restaurants or classrooms. Even in quiet environments, individuals with amblyaudia may fail to understand what they are hearing, especially if the information is new or complicated. Amblyaudia can be conceptualized as the auditory analog of the better known central visual disorder amblyopia. The term “lazy ear” has been used to describe amblyaudia although it is currently not known whether it stems from deficits in the auditory periphery or from other parts of the auditory system in the brain, or both. A characteristic of amblyaudia is suppression of activity in the non-dominant auditory pathway by activity in the dominant pathway which may be genetically determined and which could also be exacerbated by conditions throughout early development.
Deafness has varying definitions in cultural and medical contexts. In medical contexts, the meaning of deafness is hearing loss that precludes a person from understanding spoken language, an audiological condition. In this context it is written with a lower case d. It later came to be used in a cultural context to refer to those who primarily communicate through sign language regardless of hearing ability, often capitalized as Deaf and referred to as "big D Deaf" in speech and sign. The two definitions overlap but are not identical, as hearing loss includes cases that are not severe enough to impact spoken language comprehension, while cultural Deafness includes hearing people who use sign language, such as children of deaf adults.
Monita Chatterjee is an auditory scientist and the Director of the Auditory Prostheses & Perception Laboratory at Boys Town National Research Hospital. She investigates the basic mechanisms underlying auditory processing by cochlear implant listeners.
Temporal envelope (ENV) and temporal fine structure (TFS) are changes in the amplitude and frequency of sound perceived by humans over time. These temporal changes are responsible for several aspects of auditory perception, including loudness, pitch and timbre perception and spatial hearing.

Brian C.J. Moore FMedSci, FRS is an Emeritus Professor of Auditory Perception in the University of Cambridge and an Emeritus Fellow of Wolfson College, Cambridge. His research focuses on psychoacoustics, audiology, and the development and assessment of hearing aids.
Recruitment, in medicine, is a physical condition of the inner ear that leads to reduced tolerance of loudness. It commonly occurs in individuals who suffer hearing loss due to cochlear damage. While low-magnitude sounds cannot be heard in the affected ear(s), the perceived loudness increases over-proportionally with sound volume once the auditory threshold has been overcome. This can result in a reduced tolerance to loudness, as loud sounds may be perceived louder than normal.

Quentin Summerfield is a British psychologist, specialising in hearing. He joined the Medical Research Council Institute of Hearing Research in 1977 and served as its deputy director from 1993 to 2004, before moving on to a chair in psychology at The University of York. He served as head of the Psychology department from 2011 to 2017 and retired in 2018, becoming an emeritus professor. From 2013 to 2018, he was a member of the University of York's Finance & Policy Committee. From 2015 to 2018, he was a member of York University's governing body, the Council.
Sharon G. Kujawa is a clinical audiologist, Director of Audiology Research at the Massachusetts Eye and Ear Infirmary, Associate Professor of Otology and Laryngology at Harvard Medical School, and Adjunct Faculty of Harvard-MIT Health Sciences and Technology.and specialist in otolaryngology, Her specialty is the effects of noise exposure and aging on auditory function.
References
- ↑ "Mary Florentine - Speech-Language Pathology and Audiology". Archived from the original on 2010-11-16. Retrieved 2010-11-22.
- ↑ "Mary Florentine - Speech-Language Pathology and Audiology". Archived from the original on 2010-11-16. Retrieved 2010-11-22.
- ↑ http://scitation.aip.org/getpdf/servlet/GetPDFServlet?filetype=pdf&id=JASMAN000117000004001685000001&idtype=cvips&prog=normal [ dead link ]
- ↑ Florentine, Mary (2003). "It's not recruitment—gasp! It's softness imperception". The Hearing Journal. 56 (3): 10. doi: 10.1097/01.HJ.0000293012.17887.b4 . S2CID 147098933.
- ↑ Florentine, Mary; Popper, Arthur N.; Fay, Richard R. (2010-11-04). Loudness. Springer. ISBN 9781441967121.
- ↑ Florentine M, Buus S: Evidence for normal loudness growth near threshold in cochlear hearing loss. In Tranebjærg L, Christensen-Dalsgaard J, Andersen T, Poulsen T, eds. Genetics and the Function of the Auditory System. Tåstrup, Denmark: GN ReSound, 2002:411-426.
- ↑ Buus S, Florentine M: Growth of loudness in listeners with cochlear hearing losses: Recruitment reconsidered. J Assn Res Otolaryngol 2001;3:120-139.
- ↑ Florentine, Mary (2003). "It's not recruitment—gasp! It's softness imperception". The Hearing Journal. 56 (3): 10. doi: 10.1097/01.HJ.0000293012.17887.b4 . S2CID 147098933.
- ↑ Epstein, Michael; Florentine, Mary (April 2009). "Binaural loudness summation for speech and tones presented via earphones and loudspeakers". Ear Hear. 30 (2): 234–7. doi:10.1097/AUD.0b013e3181976993. PMID 19194294. S2CID 46264961.
| International | |
|---|---|
| National | |
| Other | |