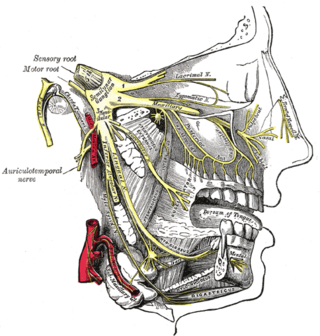
Trigeminal neuralgia, also called Fothergill disease, tic douloureux, trifacial neuralgia, or suicide disease, is a long-term pain disorder that affects the trigeminal nerve, the nerve responsible for sensation in the face and motor functions such as biting and chewing. It is a form of neuropathic pain. There are two main types: typical and atypical trigeminal neuralgia. The typical form results in episodes of severe, sudden, shock-like pain in one side of the face that lasts for seconds to a few minutes. Groups of these episodes can occur over a few hours. The atypical form results in a constant burning pain that is less severe. Episodes may be triggered by any touch to the face. Both forms may occur in the same person. It is regarded as one of the most painful disorders known to medicine, and often results in depression and suicide.

Interventional radiology (IR) is a medical specialty that performs various minimally-invasive procedures using medical imaging guidance, such as x-ray fluoroscopy, computed tomography, magnetic resonance imaging, or ultrasound. IR performs both diagnostic and therapeutic procedures through very small incisions or body orifices. Diagnostic IR procedures are those intended to help make a diagnosis or guide further medical treatment, and include image-guided biopsy of a tumor or injection of an imaging contrast agent into a hollow structure, such as a blood vessel or a duct. By contrast, therapeutic IR procedures provide direct treatment—they include catheter-based medicine delivery, medical device placement, and angioplasty of narrowed structures.
Pudendal nerve entrapment (PNE), also known as Alcock canal syndrome, is an uncommon source of chronic pain in which the pudendal nerve is entrapped or compressed in Alcock's canal. There are several different types of PNE based on the site of entrapment anatomically. Pain is positional and is worsened by sitting. Other symptoms include genital numbness, fecal incontinence and urinary incontinence.
Neuralgia is pain in the distribution of a nerve or nerves, as in intercostal neuralgia, trigeminal neuralgia, and glossopharyngeal neuralgia.
Occipital neuralgia (ON) is a painful condition affecting the posterior head in the distributions of the greater occipital nerve (GON), lesser occipital nerve (LON), third occipital nerve (TON), or a combination of the three. It is paroxysmal, lasting from seconds to minutes, and often consists of lancinating pain that directly results from the pathology of one of these nerves. It is paramount that physicians understand the differential diagnosis for this condition and specific diagnostic criteria. There are multiple treatment modalities, several of which have well-established efficacy in treating this condition.
Hemifacial spasm (HFS) is a rare neuromuscular disease characterized by irregular, involuntary muscle contractions (spasms) on one side (hemi-) of the face (-facial). The facial muscles are controlled by the facial nerve, which originates at the brainstem and exits the skull below the ear where it separates into five main branches.

The superior cerebellar artery (SCA) is an artery of the head. It arises near the end of the basilar artery. It is a branch of the basilar artery. It supplies parts of the cerebellum, the midbrain, and other nearby structures. It is the cause of trigeminal neuralgia in some patients.
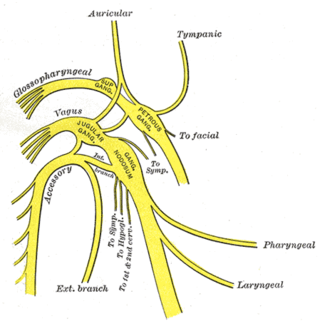
The superior ganglion of the vagus nerve is a sensory ganglion of the peripheral nervous system. It is located within the jugular foramen, where the vagus nerve exits the skull. It is smaller than and proximal to the inferior ganglion of the vagus nerve.

Decompressive craniectomy is a neurosurgical procedure in which part of the skull is removed to allow a swelling or herniating brain room to expand without being squeezed. It is performed on victims of traumatic brain injury, stroke, Chiari malformation, and other conditions associated with raised intracranial pressure. Use of this surgery is controversial.
A neurectomy, or nerve resection is a neurosurgical procedure in which a peripheral nerve is cut or removed to alleviate neuropathic pain or permanently disable some function of a nerve. The nerve is not intended to grow back. For chronic pain it may be an alternative to a failed nerve decompression when the target nerve has no motor function and numbness is acceptable. Neurectomies have also been used to permanently block autonomic function, and special sensory function not related to pain.
Hypoesthesia or numbness is a common side effect of various medical conditions that manifests as a reduced sense of touch or sensation, or a partial loss of sensitivity to sensory stimuli. In everyday speech this is generally referred to as numbness.
Geniculate ganglionitis or geniculate neuralgia (GN), also called nervus intermedius neuralgia, Ramsay Hunt syndrome, or Hunt's neuralgia, is a rare disorder characterized by severe paroxysmal neuralgic pain deep in the ear, that may spread to the ear canal, outer ear, mastoid or eye regions. GN may also occur in combination with trigeminal or glossopharyngeal neuralgia.

A laminotomy is an orthopaedic neurosurgical procedure that removes part of the lamina of a vertebral arch in order to relieve pressure in the vertebral canal. A laminotomy is less invasive than conventional vertebral column surgery techniques, such as laminectomy because it leaves more ligaments and muscles attached to the spinous process intact and it requires removing less bone from the vertebra. As a result, laminotomies typically have a faster recovery time and result in fewer postoperative complications. Nevertheless, possible risks can occur during or after the procedure like infection, hematomas, and dural tears. Laminotomies are commonly performed as treatment for lumbar spinal stenosis and herniated disks. MRI and CT scans are often used pre- and post surgery to determine if the procedure was successful.

Laminoplasty is an orthopaedic/neurosurgical surgical procedure for treating spinal stenosis by relieving pressure on the spinal cord. The main purpose of this procedure is to provide relief to patients who may have symptoms of numbness, pain, or weakness in arm movement. The procedure involves cutting the lamina on both sides of the affected vertebrae and then "swinging" the freed flap of bone open thus relieving the pressure on the spinal cord. The spinous process may be removed to allow the lamina bone flap to be swung open. The bone flap is then propped open using small wedges or pieces of bone such that the enlarged spinal canal will remain in place.
Atypical trigeminal neuralgia (ATN), or type 2 trigeminal neuralgia, is a form of trigeminal neuralgia, a disorder of the fifth cranial nerve. This form of nerve pain is difficult to diagnose, as it is rare and the symptoms overlap with several other disorders. The symptoms can occur in addition to having migraine headache, or can be mistaken for migraine alone, or dental problems such as temporomandibular joint disorder or musculoskeletal issues. ATN can have a wide range of symptoms and the pain can fluctuate in intensity from mild aching to a crushing or burning sensation, and also to the extreme pain experienced with the more common trigeminal neuralgia.

Nerve compression syndrome, or compression neuropathy, or nerve entrapment syndrome, is a medical condition caused by chronic, direct pressure on a peripheral nerve. It is known colloquially as a trapped nerve, though this may also refer to nerve root compression. Its symptoms include pain, tingling, numbness and muscle weakness. The symptoms affect just one particular part of the body, depending on which nerve is affected. The diagnosis is largely clinical and can be confirmed with diagnostic nerve blocks. Occasionally imaging and electrophysiology studies aid in the diagnosis. Timely diagnosis is important as untreated chronic nerve compression may cause permanent damage. A surgical nerve decompression can relieve pressure on the nerve but cannot always reverse the physiological changes that occurred before treatment. Nerve injury by a single episode of physical trauma is in one sense an acute compression neuropathy but is not usually included under this heading, as chronic compression takes a unique pathophysiological course.
Endoscopic endonasal surgery is a minimally invasive technique used mainly in neurosurgery and otolaryngology. A neurosurgeon or an otolaryngologist, using an endoscope that is entered through the nose, fixes or removes brain defects or tumors in the anterior skull base. Normally an otolaryngologist performs the initial stage of surgery through the nasal cavity and sphenoid bone; a neurosurgeon performs the rest of the surgery involving drilling into any cavities containing a neural organ such as the pituitary gland. The use of endoscope was first introduced in Transsphenoidal Pituitary Surgery by R Jankowsky, J Auque, C Simon et al. in 1992 G.
John Howard Sampson is an American neurosurgeon who was formerly chief of the department of neurosurgery at Duke University where he serves as a professor of surgery, biomedical engineering, immunology, and pathology.
Peter Joseph Jannetta was an American neurosurgeon known for devising microvascular decompression, a surgical procedure to treat trigeminal neuralgia. At the University of Pittsburgh School of Medicine, he was the first Walter Dandy Professor of Neurological Surgery.
A nerve decompression is a neurosurgical procedure to relieve chronic, direct pressure on a nerve to treat nerve entrapment, a pain syndrome characterized by severe chronic pain and muscle weakness. In this way a nerve decompression targets the underlying pathophysiology of the syndrome and is considered a first-line surgical treatment option for peripheral nerve pain. Despite treating the underlying cause of the disease, the symptoms may not be fully reversible as delays in diagnosis can allow permanent damage to occur to the nerve and surrounding microvasculature. Traditionally only nerves accessible with open surgery have been good candidates, however innovations in laparoscopy and nerve-sparing techniques made nearly all nerves in the body good candidates, as surgical access is no longer a barrier.