Related Research Articles
Orthodontics is a dentistry specialty that addresses the diagnosis, prevention, management, and correction of mal-positioned teeth and jaws, and misaligned bite patterns. It may also address the modification of facial growth, known as dentofacial orthopedics.

In orthodontics, a malocclusion is a misalignment or incorrect relation between the teeth of the upper and lower dental arches when they approach each other as the jaws close. The English-language term dates from 1864; Edward Angle (1855-1930), the "father of modern orthodontics", popularised it. The word "malocclusion" derives from occlusion, and refers to the manner in which opposing teeth meet.
Orthodontic technology is a specialty of dental technology that is concerned with the design and fabrication of dental appliances for the treatment of malocclusions, which may be a result of tooth irregularity, disproportionate jaw relationships, or both.

Crossbite is a form of malocclusion where a tooth has a more buccal or lingual position than its corresponding antagonist tooth in the upper or lower dental arch. In other words, crossbite is a lateral misalignment of the dental arches.

A lingual arch is an orthodontic device which connects two molars in the upper or lower dental arch. The lower lingual arch (LLA) has an archwire adapted to the lingual side of the lower teeth. In the upper arch the archwire is usually connecting the two molars passing through the palatal vault, and is commonly referred as "Transpalatal Arch" (TPA). The TPA was originally described by Robert Goshgarian in 1972. TPAs could possibly be used for maintaining transverse arch widths, anchorage in extraction case, prevent buccal tipping of molars during Burstonian segmented arch mechanics, transverse anchorage and space maintenance.
Pre-eruption guidance is an orthodontic treatment method that allows for expansion of existing erupting teeth long before they appear in the mouth. The use off pre-eruption guidance appliances and the timing of extractions of certain deciduous teeth aligns the teeth naturally as opposed to orthodontic mechanical movement of permanent teeth into alignment after they have erupted. Research shows that pre-eruption guidance produces far more stable tooth alignment than alternative treatments.
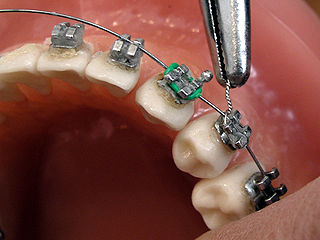
Lingual braces are one of the many types of the fixed orthodontic treatment appliances available to patients needing orthodontics. They involve attaching the orthodontic brackets on the inner sides of the teeth. The main advantage of lingual braces is their near invisibility compared to the standard braces, which are attached on the buccal (cheek) sides of the tooth. Lingual braces were invented by Craven Kurz in 1976.
Dr. Juri Kurol (1942–2011) was a Swedish orthodontist who was the president of the European Federation of Orthodontic Specialists Association until 2002. He is known for his contributions made in the field of orthodontics related to diagnosing and evaluating the eruption pattern of maxillary canines.
Dr. William J. Clark is a Scottish orthodontist known for developing Twin Block Appliance in Orthodontics. This appliance was developed by Dr. Clark in 1977 in Scotland and since then this appliance has been used in correction of Class 2 malocclusions with retrognathic mandible. He also developed invisible TransForce Appliance in 2004.

Anchorage in orthodontics is defined as a way of resisting movement of a tooth or number of teeth by using different techniques. Anchorage is an important consideration in the field of orthodontics as this is a concept that is used frequently when correcting malocclusions. Unplanned or unwanted tooth movement can have dire consequences in a treatment plan, and therefore using anchorage stop a certain tooth movement becomes important. Anchorage can be used from many different sources such as teeth, bone, implants or extra-orally.
A lip bumper is a dental appliance used in orthodontics, for various purposes to correct a dentition by preventing the pressure from the soft tissue. Lip bumpers are usually used in orthodontic treatment where the patient has a crowded maxillary or mandibular teeth in an arch.
Activator Appliance is an Orthodontics appliance that was developed by Viggo Andresen in 1908. This was one of the first functional appliances that was developed to correct functional jaw in the early 1900s. Activator appliance became the universal appliance that was used widely throughout Europe in the earlier part of the 20th century.
Frankel appliance or Frankel Functional Regulator is an orthodontic functional appliance which was developed by Rolf Fränkel in 1950s for treatment to patients of all ages. This appliance primarily focused on the modulation of neuromuscular activity in order to produce changes in jaw and teeth. The appliance was opposite to the Bionator appliance and Activator appliance.
Pendulum is an orthodontic appliance, developed by James J. Hilgers in 1992, that use forces to distalize the upper 1st molars to create space for eruption of impacted teeth or allowing correction of Class 2 malocclusion. This appliance is a fixed type of distalizing appliance that does not depend on the compliance of each patient to work. Hilgers published an article in Journal of Clinical Orthodontics in 1992 describing the appliance.
ACCO or Acrylic Cervical Occipital Anchorage is an appliance in field of orthodontics which is used for distalization of maxillary molars. This appliance is a removable type of appliance which was developed by Herbert I. Margolis. This appliance is intended to be worn 24 hours a day except during meals. It is one of the few removable appliances made for distalization of molars and thus require patient compliance for the treatment to be successful.
Failure of eruption of teeth happens when a single or multiple teeth fail to erupt in the mouth. This can happen due to many reasons which may include obstruction from primary teeth, bone surrounding the unerupted tooth or other mechanical factors. The two types of failure of eruption are primary failure of eruption and mechanical failure of eruption. Primary failure of eruption has been known to be associated with Parathyroid hormone 1 receptor mutation.
Intrusion is a movement in the field of orthodontics where a tooth is moved partially into the bone. Intrusion is done in orthodontics to correct an anterior deep bite or in some cases intrusion of the over-erupted posterior teeth with no opposing tooth. Intrusion can be done in many ways and consists of many different types. Intrusion, in orthodontic history, was initially defined as problematic in early 1900s and was known to cause periodontal effects such as root resorption and recession. However, in mid 1950s successful intrusion with light continuous forces was demonstrated. Charles J. Burstone defined intrusion to be "the apical movement of the geometric center of the root (centroid) in respect to the occlusal plane or plane based on the long axis of tooth".
Open bite is a type of orthodontic malocclusion which has been estimated to occur in 0.6% of the people in the United States. This type of malocclusion has no vertical overlap or contact between the anterior incisors. The term "open bite" was coined by Carevelli in 1842.
Anthony Gianelly (1936–2009) was an American orthodontist. He developed the bi-dimensional technique, which is widely used in various private practices of orthodontics and has been the subject of numerous publications over the years.
Orthodontic indices are one of the tools that are available for orthodontists to grade and assess malocclusion. Orthodontic indices can be useful for an epidemiologist to analyse prevalence and severity of malocclusion in any population.
References
- ↑ Sfondrini, M. F.; Cacciafesta, V.; Sfondrini, G. (2002-05-01). "Upper molar distalization: a critical analysis". Orthodontics & Craniofacial Research. 5 (2): 114–126. doi:10.1034/j.1600-0544.2002.01155.x. ISSN 1601-6335. PMID 12086326.
- ↑ William R. Proffit; Henry W. Fields Jr; David M. Sarver (2012-04-16). Contemporary Orthodontics, 5e (5 ed.). Mosby. ISBN 9780323083171.
- ↑ Graber, T. M. (1955-07-01). "Extraoral force—Facts and fallacies". American Journal of Orthodontics. 41 (7): 490–505. doi:10.1016/0002-9416(55)90143-3.
- ↑ Jeckel, Norbert; Rakosi, Thomas (1991-02-01). "Molar distalization by intra-oral force application". The European Journal of Orthodontics. 13 (1): 43–46. doi:10.1093/ejo/13.1.43. ISSN 0141-5387. PMID 2032566.
- ↑ Lim, Seung-Min; Hong, Ryoon-Ki (2009-06-29). "Distal Movement of Maxillary Molars Using a Lever-arm and Mini-implant System". The Angle Orthodontist. 78 (1): 167–175. doi: 10.2319/102506-438 . PMID 18193963.
- ↑ Muse, Dween S.; Fillman, Michael J.; William J., Emmerson; Mitchell, Robert D. (1993-12-01). "Molar and incisor changes with Wilson rapid molar distalization". American Journal of Orthodontics and Dentofacial Orthopedics. 104 (6): 556–565. doi:10.1016/S0889-5406(05)80439-1. PMID 8249931.
- 1 2 Ghosh, J.; Nanda, R. S. (1996-12-01). "Evaluation of an intraoral maxillary molar distalization technique". American Journal of Orthodontics and Dentofacial Orthopedics. 110 (6): 639–646. doi:10.1016/S0889-5406(96)80041-2. ISSN 0889-5406. PMID 8972811.
- ↑ Flores-Mir, Carlos; McGrath, Lisa; Heo, Giseon; Major, Paul W. (2013-07-01). "Efficiency of molar distalization associated with second and third molar eruption stage". The Angle Orthodontist. 83 (4): 735–742. doi: 10.2319/081612-658.1 . ISSN 1945-7103. PMC 8754030 . PMID 23167519.
- ↑ Karlsson, Ingela; Bondemark, Lars (2006-11-01). "Intraoral maxillary molar distalization". The Angle Orthodontist. 76 (6): 923–929. doi: 10.2319/110805-390 . ISSN 0003-3219. PMID 17090171.
- ↑ Bussick, T. J.; McNamara, J. A. (2000-03-01). "Dentoalveolar and skeletal changes associated with the pendulum appliance". American Journal of Orthodontics and Dentofacial Orthopedics. 117 (3): 333–343. doi:10.1016/S0889-5406(00)70238-1. ISSN 0889-5406. PMID 10715093.