Related Research Articles

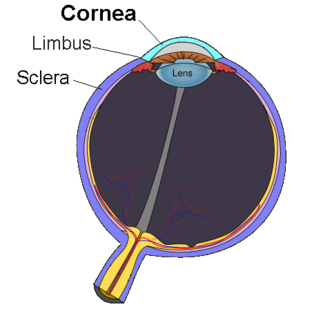
Keratitis is a condition in which the eye's cornea, the clear dome on the front surface of the eye, becomes inflamed. The condition is often marked by moderate to intense pain and usually involves any of the following symptoms: pain, impaired eyesight, photophobia, red eye and a 'gritty' sensation.
A red eye is an eye that appears red due to illness or injury. It is usually injection and prominence of the superficial blood vessels of the conjunctiva, which may be caused by disorders of these or adjacent structures. Conjunctivitis and subconjunctival hemorrhage are two of the less serious but more common causes.
Recurrent corneal erosion is a disorder of the eyes characterized by the failure of the cornea's outermost layer of epithelial cells to attach to the underlying basement membrane. The condition is excruciatingly painful because the loss of these cells results in the exposure of sensitive corneal nerves. This condition can often leave patients with temporary blindness due to extreme light sensitivity (photophobia).

Scleritis is a serious inflammatory disease that affects the white outer coating of the eye, known as the sclera. The disease is often contracted through association with other diseases of the body, such as granulomatosis with polyangiitis or rheumatoid arthritis. There are three types of scleritis: diffuse scleritis, nodular scleritis, and necrotizing scleritis. Scleritis may be the first symptom of onset of connective tissue disease.

Phlyctenular keratoconjunctivitis is an inflammatory syndrome caused by a delayed hypersensitivity reaction to one or more antigens. The triggering antigen is usually a bacterial protein, but may also be a virus, fungus, or nematode.

A corneal ulcer, or ulcerative keratitis, is an inflammatory condition of the cornea involving loss of its outer layer. It is very common in dogs and is sometimes seen in cats. In veterinary medicine, the term corneal ulcer is a generic name for any condition involving the loss of the outer layer of the cornea, and as such is used to describe conditions with both inflammatory and traumatic causes.

Vernal keratoconjunctivitis (VKC) is a recurrent, bilateral, and self-limiting inflammation of conjunctiva, having a periodic seasonal incidence.

Acanthamoeba keratitis (AK) is a rare disease in which amoebae of the genus Acanthamoeba invade the clear portion of the front (cornea) of the eye. It affects roughly 100 people in the United States each year. Acanthamoeba are protozoa found nearly ubiquitously in soil and water and can cause infections of the skin, eyes, and central nervous system.
Infectious bovine keratoconjunctivitis (IBK), also known as pinkeye, New Forest eye or blight, is a veterinary infection of cattle caused by Moraxella bovis, a Gram-negative, β-haemolytic, aerobic, rod-shaped bacterium. It is spread by direct contact or by flies serving as vectors. It is the most common ocular disease of cattle. IBK is similar to human pink eye and causes severe infection of the conjunctiva, edema, corneal opacity, and ulceration. This disease is highly contagious and occurs worldwide. Younger animals are more susceptible, but recovery with minimal damage is usual, if they are treated early.

Corneal neovascularization (CNV) is the in-growth of new blood vessels from the pericorneal plexus into avascular corneal tissue as a result of oxygen deprivation. Maintaining avascularity of the corneal stroma is an important aspect of corneal pathophysiology as it is required for corneal transparency and optimal vision. A decrease in corneal transparency causes visual acuity deterioration. Corneal tissue is avascular in nature and the presence of vascularization, which can be deep or superficial, is always pathologically related.

Corneal ulcer is an inflammatory or, more seriously, infective condition of the cornea involving disruption of its epithelial layer with involvement of the corneal stroma. It is a common condition in humans particularly in the tropics and the agrarian societies. In developing countries, children afflicted by Vitamin A deficiency are at high risk for corneal ulcer and may become blind in both eyes, which may persist lifelong. In ophthalmology, a corneal ulcer usually refers to having an infectious cause while the term corneal abrasion refers more to physical abrasions.

Chronic superficial keratitis (CSK), also known as pannus or Uberreiter's disease, is an inflammatory condition of the cornea in dogs, particularly seen in the German Shepherd. Both eyes are usually affected. The corneas gradually become pigmented and infiltrated by blood vessels, and the dog may eventually become blind.

Corneal dystrophies are a group of diseases that affect the cornea in dogs.

Herpetic simplex keratitis is a form of keratitis caused by recurrent herpes simplex virus (HSV) infection in the cornea.
Mooren's ulcer is a rare idiopathic ocular disorder that may lead to blindness due to progressive destruction of the peripheral cornea. Although the etiology of Mooren's ulcer is poorly understood, recent evidence suggests that the pathogenesis of this disease appears to be the result of an autoimmune process directed against molecules expressed in the corneal stroma.
Neurotrophic keratitis (NK) is a degenerative disease of the cornea caused by damage of the trigeminal nerve, which results in impairment of corneal sensitivity, spontaneous corneal epithelium breakdown, poor corneal healing and development of corneal ulceration, melting and perforation. This is because, in addition to the primary sensory role, the nerve also plays a role maintaining the integrity of the cornea by supplying it with trophic factors and regulating tissue metabolism.

Virender Singh Sangwan is an Indian ophthalmologist and the Dr. Paul Dubord Chair professor and director of the L. V. Prasad Eye Institute, Hyderabad. Known for his research on limbal stem cells, Sangwan is the founder secretary and an adviser of the Uveitis Society of India. The Council of Scientific and Industrial Research, the apex agency of the Government of India for scientific research, awarded him the Shanti Swarup Bhatnagar Prize for Science and Technology, one of the highest Indian science awards for his contributions to Medical Sciences in 2006.

The human cornea is a transparent membrane which allows light to pass through it. The word corneal opacification literally means loss of normal transparency of cornea. The term corneal opacity is used particularly for the loss of transparency of cornea due to scarring. Transparency of the cornea is dependent on the uniform diameter and the regular spacing and arrangement of the collagen fibrils within the stroma. Alterations in the spacing of collagen fibrils in a variety of conditions including corneal edema, scars, and macular corneal dystrophy is clinically manifested as corneal opacity. The term corneal blindness is commonly used to describe blindness due to corneal opacity.
Exposure keratopathy is medical condition affecting the cornea of eyes. It can lead to corneal ulceration and permanent loss of vision due to corneal opacity.
Topical prednisolone is a type of glucocorticoid, mainly used in the ophthalmic pathway as eye drops in numerous eye conditions, such as corneal injuries caused by chemicals, burns and alien objects, inflammation of the eyes, mild to moderate non-infectious allergies, disorders of the eyelid, conjunctiva or sclera, ocular inflammation caused by operation and optic neuritis. Some side effects include glaucoma, blurring of vision, eye discomfort, impaired recovery of injured site, scarring of the optic nerve, clouding of lenses and urticaria. However, their prevalence is not known.
References
- 1 2 3 4 5 6 7 8 Devi, Saranya; Sethi, Anin; Gupta, Noopur; Sen, Seema; Vanathi, M. (2017), Tandon, Radhika; Galor, Anat; Sangwan, Virender Singh; Ray, Manotosh (eds.), "Anatomical Considerations", Peripheral Ulcerative Keratitis, Cham: Springer International Publishing, pp. 3–9, doi:10.1007/978-3-319-50404-9_1, ISBN 978-3-319-50402-5 , retrieved 2021-04-01
- 1 2 3 4 Ng, Ellen Yu-Keh (2020-05-08). "Peripheral Ulcerative Keratitis: Background, Pathophysiology, Epidemiology".
{{cite journal}}: Cite journal requires|journal=(help) - 1 2 Pelegrin, L.; Hernández-Rodríguez, J.; Torras, J.; Espinosa, G.; Adán, A.; Sainz, M.T. (June 2018). "AB0678 Peripheral ulcerative keratitis associated to autoimmune systemic diseases: visual prognosis and occurrence while systemic disease in remission". Vasculitis. BMJ Publishing Group Ltd and European League Against Rheumatism: 1482.3–1483. doi: 10.1136/annrheumdis-2018-eular.4334 .
- 1 2 3 4 Efron, Nathan (2019). Contact lens complications (Fourth ed.). Philadelphia, PA. ISBN 978-0-7020-7882-8. OCLC 1076544647.
- 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 Maharana, Prafulla K.; Pattebahadur, Rajesh; Sharma, Namrata (2017), Tandon, Radhika; Galor, Anat; Sangwan, Virender Singh; Ray, Manotosh (eds.), "Clinical Evaluation", Peripheral Ulcerative Keratitis, Cham: Springer International Publishing, pp. 17–25, doi:10.1007/978-3-319-50404-9_3, ISBN 978-3-319-50402-5 , retrieved 2021-04-01
- 1 2 3 4 5 6 7 8 9 10 11 12 Singh, Divya; Galor, Anat; Tandon, Radhika (2017), Tandon, Radhika; Galor, Anat; Sangwan, Virender Singh; Ray, Manotosh (eds.), "Investigative Modalities", Peripheral Ulcerative Keratitis, Cham: Springer International Publishing, pp. 27–34, doi:10.1007/978-3-319-50404-9_4, ISBN 978-3-319-50402-5 , retrieved 2021-04-01
- 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 Yanoff, Myron; Duker, Jay S (2018). Ophthalmology (Fifth ed.). Edinburgh: Elsevier Health Sciences. ISBN 978-0-323-52821-4. OCLC 1051774434.
- 1 2 Ogra, Siddharth; Sims, Joanne L.; McGhee, Charles N. J.; Niederer, Rachael L. (May 2020). "Ocular complications and mortality in peripheral ulcerative keratitis and necrotising scleritis: The role of systemic immunosuppression". Clinical & Experimental Ophthalmology. 48 (4): 434–441. doi:10.1111/ceo.13709. ISSN 1442-6404. PMID 31872475. S2CID 209462208.
- 1 2 3 4 5 6 7 8 9 Murray, Philip Ian; Rauz, Saaeha (2016). "The eye and inflammatory rheumatic diseases: The eye and rheumatoid arthritis, ankylosing spondylitis, psoriatic arthritis". Best Practice & Research. Clinical Rheumatology. 30 (5): 802–825. doi:10.1016/j.berh.2016.10.007. ISSN 1532-1770. PMID 27964790.
- 1 2 3 4 5 6 7 Gomes, Beatriz Fiuza; Santhiago, Marcony R. (March 2021). "Biology of peripheral ulcerative keratitis". Experimental Eye Research. 204: 108458. doi:10.1016/j.exer.2021.108458. PMID 33493475. S2CID 231710506.
- 1 2 3 4 5 Lohchab, Monica; Prakash, Gaurav; Arora, Tarun; Maharana, Prafulla; Jhanji, Vishal; Sharma, Namrata; Vajpayee, Rasik B. (January 2019). "Surgical management of peripheral corneal thinning disorders". Survey of Ophthalmology. 64 (1): 67–78. doi:10.1016/j.survophthal.2018.06.002. ISSN 1879-3304. PMID 29886126. S2CID 47007321.
- ↑ Açıkalın, Banu (2018). "Clinical findings, pathogenesis and treatment in non-infectious peripheral ulcerative keratitis". Beyoglu Eye Journal. 3 (2). doi: 10.14744/bej.2018.10820 .
- ↑ Antoun, Joëlle; Titah, Cherif; Cochereau, Isabelle (2016). "Ocular and orbital side-effects of checkpoint inhibitors: a review article". Current Opinion in Oncology. 28 (4): 288–294. doi:10.1097/CCO.0000000000000296. ISSN 1531-703X. PMID 27136135. S2CID 19600151.
- 1 2 3 4 5 6 7 8 9 10 11 Deshmukh, Rashmi; Stevenson, Louis J.; Vajpayee, Rasik B. (2020). "Techniques of noncircular corneal transplantation". Current Opinion in Ophthalmology. 31 (4): 293–301. doi:10.1097/ICU.0000000000000672. ISSN 1040-8738. PMID 32412959. S2CID 218659155.
- 1 2 Cao, Yan; Zhang, Wensong; Wu, Jie; Zhang, Hong; Zhou, Hongyan (2017-07-13). "Peripheral Ulcerative Keratitis Associated with Autoimmune Disease: Pathogenesis and Treatment". Journal of Ophthalmology. 2017: 1–12. doi: 10.1155/2017/7298026 . PMC 5530438 . PMID 28785483.
- 1 2 3 4 5 6 Ray, Manotosh; Chan, Hwei Wuen (2017), Tandon, Radhika; Galor, Anat; Sangwan, Virender Singh; Ray, Manotosh (eds.), "Etiopathogenesis", Peripheral Ulcerative Keratitis, Cham: Springer International Publishing, pp. 11–15, doi:10.1007/978-3-319-50404-9_2, ISBN 978-3-319-50402-5 , retrieved 2021-04-01
- 1 2 Yagci, Ayse (2012). "Update on peripheral ulcerative keratitis". Clinical Ophthalmology. 6: 747–754. doi:10.2147/OPTH.S24947. ISSN 1177-5483. PMC 3363308 . PMID 22654502.
- 1 2 3 4 5 6 Tandon, Radhika; Singh, Archita; Sangwan, Virender Singh (2017), Tandon, Radhika; Galor, Anat; Sangwan, Virender Singh; Ray, Manotosh (eds.), "General Principles of Medical Therapy", Peripheral Ulcerative Keratitis, Cham: Springer International Publishing, pp. 35–49, doi:10.1007/978-3-319-50404-9_5, ISBN 978-3-319-50402-5 , retrieved 2021-04-01