
Kidney cancer, also known as renal cancer, is a group of cancers that starts in the kidney. Symptoms may include blood in the urine, lump in the abdomen, or back pain. Fever, weight loss, and tiredness may also occur. Complications can include spread to the lungs or brain.

Malignancy is the tendency of a medical condition to become progressively worse; the term is most familiar as a characterization of cancer.
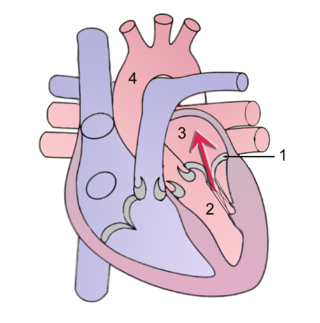
Mitral regurgitation(MR), also known as mitral insufficiency or mitral incompetence, is a form of valvular heart disease in which the mitral valve is insufficient and does not close properly when the heart pumps out blood. It is the abnormal leaking of blood backwards – regurgitation from the left ventricle, through the mitral valve, into the left atrium, when the left ventricle contracts. Mitral regurgitation is the most common form of valvular heart disease.

A myxoma is a myxoid tumor of primitive connective tissue. It is most commonly found in the heart but can also occur in other locations.

A rhabdomyoma is a benign tumor of striated muscle. Rhabdomyomas may be either cardiac or extracardiac. Extracardiac forms of rhabdomyoma are sub-classified into three distinct types: adult type, fetal type, and genital type.
Libman–Sacks endocarditis is a form of non-bacterial endocarditis that is seen in association with systemic lupus erythematosus, antiphospholipid syndrome, and malignancies. It is one of the most common cardiac manifestations of lupus.
Spinal tumors are neoplasms located in either the vertebral column or the spinal cord. There are three main types of spinal tumors classified based on their location: extradural and intradural. Extradural tumors are located outside the dura mater lining and are most commonly metastatic. Intradural tumors are located inside the dura mater lining and are further subdivided into intramedullary and extramedullary tumors. Intradural-intramedullary tumors are located within the dura and spinal cord parenchyma, while intradural-extramedullary tumors are located within the dura but outside the spinal cord parenchyma. The most common presenting symptom of spinal tumors is nocturnal back pain. Other common symptoms include muscle weakness, sensory loss, and difficulty walking. Loss of bowel and bladder control may occur during the later stages of the disease.

Angiosarcoma is a rare and aggressive cancer that starts in the endothelial cells that line the walls of blood vessels or lymphatic vessels. Since they are made from vascular lining, they can appear anywhere and at any age, but older people are more commonly affected, and the skin is the most affected area, with approximately 60% of cases being cutaneous. Specifically, the scalp makes up ~50% of angiosarcoma cases, but this is still <0.1% of all head and neck tumors. Since angiosarcoma is an umbrella term for many types of tumor that vary greatly in origin and location, many symptoms may occur, from completely asymptomatic to non-specific symptoms like skin lesions, ulceration, shortness of breath and abdominal pain. Multiple-organ involvement at time of diagnosis is common and makes it difficult to ascertain origin and how to treat it.

Superior vena cava syndrome (SVCS), is a group of symptoms caused by obstruction of the superior vena cava ("SVC"), a short, wide vessel carrying circulating blood into the heart. The majority of cases are caused by malignant tumors within the mediastinum, most commonly lung cancer and non-Hodgkin's lymphoma, directly compressing or invading the SVC wall. Non-malignant causes are increasing in prevalence due to expanding use of intravascular devices, which can result in thrombosis. Other non-malignant causes include benign mediastinal tumors, aortic aneurysm, infections, and fibrosing mediastinitis.

A carcinoid is a slow-growing type of neuroendocrine tumor originating in the cells of the neuroendocrine system. In some cases, metastasis may occur. Carcinoid tumors of the midgut are associated with carcinoid syndrome.
The International Classification of Diseases for Oncology (ICD-O) is a domain-specific extension of the International Statistical Classification of Diseases and Related Health Problems for tumor diseases. This classification is widely used by cancer registries.

Hemangioendotheliomas are a family of vascular neoplasms of intermediate malignancy.
Carcinoid syndrome is a paraneoplastic syndrome comprising the signs and symptoms that occur secondary to neuroendocrine tumors. The syndrome is caused by neuroendocrine tumors most often found in the gut releasing biologically active substances into the blood causing symptoms such as flushing and diarrhea, and less frequently, heart failure, vomiting and bronchoconstriction.

A pericardial effusion is an abnormal accumulation of fluid in the pericardial cavity. The pericardium is a two-part membrane surrounding the heart: the outer fibrous connective membrane and an inner two-layered serous membrane. The two layers of the serous membrane enclose the pericardial cavity between them. This pericardial space contains a small amount of pericardial fluid, normally 15-50 mL in volume. The pericardium, specifically the pericardial fluid provides lubrication, maintains the anatomic position of the heart in the chest, and also serves as a barrier to protect the heart from infection and inflammation in adjacent tissues and organs.
Heart cancer is an extremely rare form of cancer that is divided into primary tumors of the heart and secondary tumors of the heart.
A myxoma is a rare benign tumor of the heart. Myxomata are the most common primary cardiac tumor in adults, and are most commonly found within the left atrium near the valve of the fossa ovalis. Myxomata may also develop in the other heart chambers. The tumor is derived from multipotent mesenchymal cells. Cardiac myxoma can affect adults between 30 and 60 years of age.

Transitional cell carcinoma, also called urothelial carcinoma, is a type of cancer that typically occurs in the urinary system. It is the most common type of bladder cancer and cancer of the ureter, urethra, and urachus. Symptoms of urothelial carcinoma in the bladder include hematuria. Diagnosis includes urine analysis and imaging of the urinary tract (cystoscopy). Transitional cell carcinomas arise from the transitional epithelium, a tissue lining the inner surface of these hollow organs. When the term "urothelial" is used, it specifically refers to a carcinoma of the urothelium, meaning a transitional cell carcinomas of the urinary system.

A papillary fibroelastoma is a primary tumor of the heart that typically involves one of the valves of the heart. Papillary fibroelastomas, while considered uncommon, make up about 10 percent of all primary tumors of the heart. They are the third most common type of primary tumor of the heart, behind cardiac myxomas and cardiac lipomas.
Cardiac fibroma, also known as cardiac fibromatosis, cardiac fibrous hamartoma, fibroelastic hamartoma of heart and fibroma of heart is the second highest type of primary cardiac tumor seen in infants and children. This benign tumor made by connective tissue and fibroblast is largely observed in the ventricles of the heart. The left ventricle is the most common location of cardiac fibroma and accounts for approximately 57% of cardiac fibroma cases followed by the right ventricle with 27.5% of cases. Symptoms of the disease depend on the size of the tumor, its location relative to the conduction system, and whether it obstructs blood flow. Two-thirds of children with this tumor are asymptomatic, showing no signs and symptoms. Therefore the cause of cardiac fibroma is unexplained but has been associated with Gorlin Syndrome. Echocardiography is the primarily diagnostic method used to detect if an individual has cardiac fibroma. Resection of the tumor is recommended however heart transplantation is done if surgery is not possible. Overall prognosis of resection is favorable and the chance of recurrence is scarcely reported.
Hyperthermic intrathoracic chemotherapy (HITOC) is part of a surgical strategy employed in the treatment of various pleural malignancies. The pleura in this situation could be considered to include the surface linings of the chest wall, lungs, mediastinum, and diaphragm. HITOC is the chest counterpart of HIPEC. Traditionally used in the treatment of malignant mesothelioma, a primary malignancy of the pleura, this modality has recently been evaluated in the treatment of secondary pleural malignancies.

