Related Research Articles

Endodontics is the dental specialty concerned with the study and treatment of the dental pulp.

Toothache, also known as dental pain, is pain in the teeth or their supporting structures, caused by dental diseases or pain referred to the teeth by non-dental diseases. When severe it may impact sleep, eating, and other daily activities.

The pulp is the part in the center of a tooth made up of living connective tissue and cells called odontoblasts. The pulp is a part of the dentin–pulp complex (endodontium). The vitality of the dentin-pulp complex, both during health and after injury, depends on pulp cell activity and the signaling processes that regulate the cell's behavior.

Deciduous teeth – commonly known as baby teeth, milk teeth, temporary teeth, and primary teeth – are the first set of teeth in the growth and development of humans and other diphyodont mammals. They develop during the embryonic stage of development and erupt during infancy. They are usually lost and replaced by permanent teeth, but in the absence of their permanent replacements, they can remain functional for many years into adulthood.
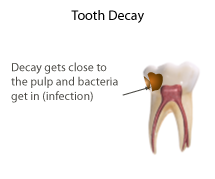
Pulpitis is inflammation of dental pulp tissue. The pulp contains the blood vessels, the nerves, and connective tissue inside a tooth and provides the tooth’s blood and nutrients. Pulpitis is mainly caused by bacterial infection which itself is a secondary development of caries. It manifests itself in the form of a toothache.

Veterinary dentistry is the field of dentistry applied to the care of animals. It is the art and science of prevention, diagnosis, and treatment of conditions, diseases, and disorders of the oral cavity, the maxillofacial region, and its associated structures as it relates to animals.

Dentigerous cyst, also known as follicular cyst is an epithelial-lined developmental cyst formed by accumulation of fluid between the reduced enamel epithelium and crown of an unerupted tooth. It is formed when there is an alteration in the reduced enamel epithelium and encloses the crown of an unerupted tooth at the cemento-enamel junction. Fluid is accumulated between reduced enamel epithelium and the crown of an unerupted tooth. Dentigerous cyst is the second most common form of benign developmental odontogenic cysts.

Commonly known as a dental cyst, the periapical cyst is the most common odontogenic cyst. It may develop rapidly from a periapical granuloma, as a consequence of untreated chronic periapical periodontitis.

Root canal treatment is a treatment sequence for the infected pulp of a tooth which is intended to result in the elimination of infection and the protection of the decontaminated tooth from future microbial invasion. Root canals, and their associated pulp chamber, are the physical hollows within a tooth that are naturally inhabited by nerve tissue, blood vessels and other cellular entities. Together, these items constitute the dental pulp.
Apical periodontitis is typically the body's defense response to the threat of microbial invasion from the root canal. Primary among the members of the host defense mechanism is the polymorphonuclear leukocyte, otherwise known as the neutrophil. The task of the neutrophil is to locate and destroy microbes that intrude into the body – anywhere in the body – and they represent the hallmark of acute inflammation.
Pulpotomy is a minimally invasive procedure performed in children on a primary tooth with extensive caries but without evidence of root pathology. The minimally invasive endodontic techniques of vital pulp therapy (VPT) are based on improved understanding of the capacity of pulp (nerve) tissues to heal and regenerate plus the availability of advanced endodontic materials. During the caries removal, this results in a carious or mechanical pulp exposure (bleeding) from the cavity. During pulpotomy, the inflamed/diseased pulp tissue is removed from the coronal pulp chamber of the tooth leaving healthy pulp tissue which is dressed with a long-term clinically-successful medicament that maintains the survival of the pulp and promotes repair. There are various types of medicament placed above the vital pulp such as Buckley’s Solution of formocresol, ferric sulfate, calcium hydroxide or MTA. MTA is a more recent material used for pulpotomies with a high rate of success, better than formocresol or ferric sulfate. It is also recommended to be the preferred pulpotomy agent in the future. After the coronal pulp chamber is filled, the tooth is restored with a filling material that seals the tooth from microleakage, such as a stainless steel crown which is the most effective long-term restoration. However, if there is sufficient remaining supporting tooth structure, other filling materials such as amalgam or composite resin can provide a functional alternative when the primary tooth has a life span of two years or less. The medium- to long-term treatment outcomes of pulpotomy in symptomatic permanent teeth with caries, especially in young people, indicate that pulpotomy can be a potential alternative to root canal therapy (RCT).
Tooth resorption, or root resorption, is the progressive loss of dentine and cementum by the action of osteoclasts. This is a normal physiological process in the exfoliation of the primary dentition, caused by osteoclast differentiation due to pressure exerted by the erupting permanent tooth. However, in the secondary dentition the process is pathological.
Pulp necrosis is a clinical diagnostic category indicating the death of the pulp and nerves of the pulp chamber and root canal of a tooth which may be due to bacterial sequelae, trauma and chemical or mechanical irritation. It is often the end result of many cases of dental trauma, caries and irreversible pulpitis.
Dental pulpal testing is a clinical and diagnostic aid used in dentistry to help establish the health of the dental pulp within the pulp chamber and root canals of a tooth. Such investigations are important in aiding dentists in devising a treatment plan for the tooth being tested.

Pulp stones are nodular, calcified masses appearing in either or both the coronal and root portion of the pulp organ in teeth. Pulp stones are not painful unless they impinge on nerves.

Periapical periodontitis or apical periodontitis (AP) is an acute or chronic inflammatory lesion around the apex of a tooth root, most commonly caused by bacterial invasion of the pulp of the tooth. It is a likely outcome of untreated dental caries, and in such cases it can be considered a sequela in the natural history of tooth decay, irreversible pulpitis and pulpal necrosis. Other causes can include occlusal trauma due to 'high spots' after restoration work, extrusion from the tooth of root filling material, or bacterial invasion and infection from the gums. Periapical periodontitis may develop into a periapical abscess, where a collection of pus forms at the end of the root, the consequence of spread of infection from the tooth pulp, or into a periapical cyst, where an epithelial lined, fluid-filled structure forms.
The Hall Technique is a non-invasive treatment for decayed baby back (molar) teeth. Decay is sealed under preformed crowns, avoiding injections and drilling. It is one of a number of biologically orientated strategies for managing dental decay.

Regenerative endodontic procedures (REPS) is defined as biologically based procedures designed to replace damaged structures such as dentin, root structures, and cells of the pulp-dentin complex. This new treatment modality aims to promote normal function of the pulp. It has become an alternative to heal apical periodontitis. Regenerative endodontics is the extension of root canal therapy. Conventional root canal therapy cleans and fills the pulp chamber with biologically inert material after destruction of the pulp due to dental caries, congenital deformity or trauma. Regenerative endodontics instead seeks to replace live tissue in the pulp chamber. The ultimate goal of REPS is to regenerate the tissues and the normal function of the dentin-pulp complex.

Pulp capping is a technique used in dental restorations to prevent the dental pulp from necrosis, after being exposed, or nearly exposed during a cavity preparation, from a traumatic injury, or by a deep cavity that reaches the center of the tooth causing the pulp to die. When dental caries is removed from a tooth, all or most of the infected and softened enamel and dentin are removed. This can lead to the pulp of the tooth either being exposed or nearly exposed which causes pulpitis (inflammation). Pulpitis, in turn, can become irreversible, leading to pain and pulp necrosis, and necessitating either root canal treatment or extraction. The ultimate goal of pulp capping or stepwise caries removal is to protect a healthy dental pulp and avoid the need for root canal therapy.
Periapical granuloma, also sometimes referred to as a radicular granuloma or apical granuloma, is an inflammation at the tip of a dead (nonvital) tooth. It is a lesion or mass that typically starts out as an epithelial lined cyst, and undergoes an inward curvature that results in inflammation of granulation tissue at the root tips of a dead tooth. This is usually due to dental caries or a bacterial infection of the dental pulp. Periapical granuloma is an infrequent disorder that has an occurrence rate between 9.3 to 87.1 percent. Periapical granuloma is not a true granuloma due to the fact that it does not contain granulomatous inflammation; however, periapical granuloma is a common term used.
References
- 1 2 3 Anilkumar K, Lingeswaran S, Ari G, Thyagarajan R, Logaranjani A (January 2016). "Management of Chronic Hyperplastic Pulpitis in Mandibular Molars of Middle Aged Adults- A Multidisciplinary Approach". Journal of Clinical and Diagnostic Research. 10 (1): ZD23-5. doi:10.7860/JCDR/2016/15338.7153. PMC 4740721 . PMID 26894192.
- 1 2 Suresh K, Bajaj N, Nayak A, Chapi D, Patil S, Rani A (January 2015). "Pulp polyp-A periapical lesion: Radiographic observational study". Journal of Indian Academy of Oral Medicine and Radiology. 27 (1): 68. doi: 10.4103/0972-1363.167085 .
- 1 2 Purkait SK (2011). Essentials of oral pathology (3rd ed.). New Delhi: Jaypee Bros. Medical Publishers. ISBN 9789350252147. OCLC 800625714.
- ↑ Chandra S, Chandra S, Chandra G, Kamala R (2007). Oral medicine. New Delhi: Jaypee Brothers Medical Publishers. ISBN 9788184481457. OCLC 704646591.
- ↑ Ingle JI, Bakland LK (2002). Endodontics (5th ed.). Hamilton: Decker. ISBN 9781550091885. OCLC 51764664.
- ↑ Torabinejad M, Walton RE, Fouad AF (2015). Endodontics : principles and practice (Fifth ed.). St. Louis, Mo.: Elsevier. ISBN 9780323225342. OCLC 935231526.