
Borderline personality disorder (BPD), also known as emotionally unstable personality disorder (EUPD), is a personality disorder characterized by a long-term pattern of intense and unstable interpersonal relationships, distorted sense of self, and strong emotional reactions. Those affected often engage in self-harm and other dangerous behaviors, often due to their difficulty with returning their emotional level to a healthy or normal baseline. They may also struggle with a feeling of emptiness, fear of abandonment, and dissociation.

Self-harm is intentional behavior that is considered harmful to oneself. This is most commonly regarded as direct injury of one's own skin tissues usually without a suicidal intention. Other terms such as cutting, self-injury, and self-mutilation have been used for any self-harming behavior regardless of suicidal intent. Common forms of self-harm include damaging the skin with a sharp object or by scratching, hitting, or burning. The exact bounds of self-harm are imprecise, but generally exclude tissue damage that occurs as an unintended side-effect of eating disorders or substance abuse, as well as societally acceptable body modification such as tattoos and piercings.
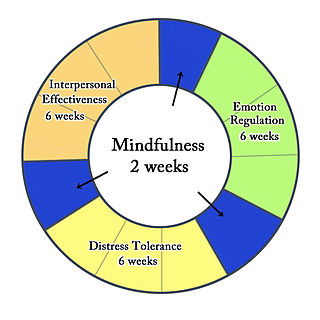
Dialectical behavior therapy (DBT) is an evidence-based psychotherapy that began with efforts to treat personality disorders and interpersonal conflicts. Evidence suggests that DBT can be useful in treating mood disorders and suicidal ideation as well as for changing behavioral patterns such as self-harm and substance use. DBT evolved into a process in which the therapist and client work with acceptance and change-oriented strategies and ultimately balance and synthesize them—comparable to the philosophical dialectical process of thesis and antithesis, followed by synthesis.
Self-hatred is personal self-loathing or hatred of oneself, or low self-esteem which may lead to self-harm.

Suicide prevention is a collection of efforts to reduce the risk of suicide. Suicide is often preventable, and the efforts to prevent it may occur at the individual, relationship, community, and society level. Suicide is a serious public health problem that can have long-lasting effects on individuals, families, and communities. Preventing suicide requires strategies at all levels of society. This includes prevention and protective strategies for individuals, families, and communities. Suicide can be prevented by learning the warning signs, promoting prevention and resilience, and committing to social change.

Excoriation disorder, more commonly known as dermatillomania, is a mental disorder on the obsessive–compulsive spectrum that is characterized by the repeated urge or impulse to pick at one's own skin, to the extent that either psychological or physical damage is caused.
Relational aggression, alternative aggression, or relational bullying is a type of aggression in which harm is caused by damaging someone's relationships or social status.
Irritability is the excitatory ability that living organisms have to respond to changes in their environment. The term is used for both the physiological reaction to stimuli and for the pathological, abnormal or excessive sensitivity to stimuli.

Suicidal ideation, or suicidal thoughts, is the thought process of having ideas, or ruminations about the possibility of ending one's own life. It is not a diagnosis but is a symptom of some mental disorders, use of certain psychoactive drugs, and can also occur in response to adverse life events without the presence of a mental disorder.
Emotion dysregulation is a range of emotional responses that do not lie within a desirable scope of emotive response, considering the stimuli.
Autophagia refers to the practice of biting/consuming one's body. It is a sub category of self-injurious behavior (SIB). Commonly, it manifests in humans as nail biting and hair pulling. In rarer circumstances, it manifests as serious self mutilative behavior such as biting of one's fingers. Autophagia affects both humans and non humans. Human autophagia typically occurs in parts of the body that are sensitive to pain, such as fingers. Human autophagia is not motivated by suicidal intent, but may be related to the desire to seek pain.

Self-destructive behavior is any behavior that is harmful or potentially harmful towards the person who engages in the behavior.
Armando Favazza is an American author and psychiatrist best known for his studies of cultural psychiatry, deliberate self-harm, and religion. Favazza's Bodies Under Siege: Self-mutilation in Culture and Psychiatry (1987) was an early psychiatric book on this topic. His 2004 work, PsychoBible: Behavior, Religion, and the Holy Book presents objective data regarding commonly held misconceptions about the Bible as a whole as well as its major passages. In Kaplan and Sadock's Comprehensive Textbook of Psychiatry he has written the chapter on "Anthropology and Psychiatry" in the 3rd edition (1980), the 4th edition (1985) and the 8th edition (2005), as well as the chapter on "Spirituality and Psychiatry" in the 9th edition (2009). He has published two cover articles in the American Journal of Psychiatry: "Foundations of Cultural Psychiatry" [135:293-303,1978] and "Modern Christian Healing of Mental Illness" [139:728-735,1982]. In 1979 he co-founded The Society for the Study of Culture and Psychiatry.

Suicide is the act of intentionally causing one's own death. Mental disorders, physical disorders, and substance abuse are risk factors. Some suicides are impulsive acts due to stress, relationship problems, or harassment and bullying. Those who have previously attempted suicide are at a higher risk for future attempts. Effective suicide prevention efforts include limiting access to methods of suicide such as firearms, drugs, and poisons; treating mental disorders and substance abuse; careful media reporting about suicide; and improving economic conditions. Although crisis hotlines are common resources, their effectiveness has not been well studied.
A suicide attempt is an act in which an individual tries to die by suicide but survives. While it may be described as a "failed" or "unsuccessful" suicide attempt, mental health professionals discourage the use of these terms as they imply that a suicide resulting in death is a successful or desirable outcome.

The Columbia Suicide Severity Rating Scale, or C-SSRS, is a suicidal ideation and behavior rating scale created by researchers at Columbia University, University of Pennsylvania, University of Pittsburgh and New York University to evaluate suicide risk. It rates an individual's degree of suicidal ideation on a scale, ranging from "wish to be dead" to "active suicidal ideation with specific plan and intent and behaviors." Questions are phrased for use in an interview format, but the C-SSRS may be completed as a self-report measure if necessary. The scale identifies specific behaviors which may be indicative of an individual's intent to kill oneself. An individual exhibiting even a single behavior identified by the scale was 8 to 10 times more likely to die by suicide.
Historically, suicide terminology has been rife with issues of nomenclature, connotation, and outcomes, and terminology describing suicide has often been defined differently depending on the purpose of the definition. A lack of agreed-upon nomenclature and operational definitions has complicated understanding. In 2007, attempts were made to reach some consensus. There is also opposition to the phrase "to commit suicide" as implying negative moral judgment and association with criminal or sinful activity.
The Suicide Behaviors Questionnaire-Revised (SBQ-R) is a psychological self-report questionnaire designed to identify risk factors for suicide in children and adolescents between ages 13 and 18. The four-question test is filled out by the child and takes approximately five minutes to complete. The questionnaire has been found to be reliable and valid in recent studies. One study demonstrated that the SBQ-R had high internal consistency with a sample of university students. However, another body of research, which evaluated some of the most commonly used tools for assessing suicidal thoughts and behaviors in college-aged students, found that the SBQ-R and suicide assessment tools in general have very little overlap between them. One of the greatest strengths of the SBQ-R is that, unlike some other tools commonly used for suicidality assessment, it asks about future anticipation of suicidal thoughts or behaviors as well as past and present ones and includes a question about lifetime suicidal ideation, plans to commit suicide, and actual attempts.
Theodore P. Beauchaine is an American psychologist and William K. Warren Foundation Professor of Psychology at the University of Notre Dame. His research focuses on neural bases of behavioral impulsivity, emotion dysregulation, and self-injurious behavior, and how these neural vulnerabilities interact with environmental risk factors across development for both boys and girls. He is among the first psychologists to specify how impulsivity, expressed early in life as ADHD, follows different developmental trajectories across the lifespan for boys vs. girls who are exposed to adversity. In contexts of maltreatment, deviant peer affiliations, and other environment risk factors, boys with ADHD are more likely to develop conduct problems, substance use disorders, and antisocial traits, whereas girls with ADHD are more likely to engage in self-injurious behavior and develop borderline traits. In protective environments, these outcomes are far less likely. Beauchaine has received two awards from the American Psychological Association: the Distinguished Scientific Award for an Early Career Contribution to Psychology and the Mid-Career Award for Outstanding Contributions to Benefit Children, Youth, and Families.
A self-inflicted wound (SIW) or self-inflicted injury (SII) is a physical injury done to oneself. This may occur in contexts including:

