Related Research Articles
Sinusitis, also known as rhinosinusitis, is inflammation of the mucous membranes that line the sinuses resulting in symptoms that may include thick nasal mucus, a plugged nose, and facial pain. Other signs and symptoms may include fever, headaches, a poor sense of smell, sore throat, a feeling that phlegm is oozing out from the back of the nose to the throat along with a necessity to clear the throat frequently and frequent attacks of cough.

Cholesteatoma is a destructive and expanding growth consisting of keratinizing squamous epithelium in the middle ear and/or mastoid process. Cholesteatomas are not cancerous as the name may suggest, but can cause significant problems because of their erosive and expansile properties. This can result in the destruction of the bones of the middle ear (ossicles), as well as growth through the base of the skull into the brain. They often become infected and can result in chronically draining ears. Treatment almost always consists of surgical removal.

Nasal polyps (NP) are noncancerous growths within the nose or sinuses. Symptoms include trouble breathing through the nose, loss of smell, decreased taste, post nasal drip, and a runny nose. The growths are sac-like, movable, and nontender, though face pain may occasionally occur. They typically occur in both nostrils in those who are affected. Complications may include sinusitis and broadening of the nose.

Diplopia is the simultaneous perception of two images of a single object that may be displaced horizontally or vertically in relation to each other. Also called double vision, it is a loss of visual focus under regular conditions, and is often voluntary. However, when occurring involuntarily, it results in impaired function of the extraocular muscles, where both eyes are still functional, but they cannot turn to target the desired object. Problems with these muscles may be due to mechanical problems, disorders of the neuromuscular junction, disorders of the cranial nerves that innervate the muscles, and occasionally disorders involving the supranuclear oculomotor pathways or ingestion of toxins.

The pyramid-shaped maxillary sinus is the largest of the paranasal sinuses, located in the maxilla. It drains into the middle meatus of the nose through the semilunar hiatus. It is located to the side of the nasal cavity, and below the orbit.
Balloon sinuplasty is a procedure that ear, nose and throat surgeons may use for the treatment of blocked sinuses. Patients diagnosed with sinusitis but not responding to medications may be candidates for sinus surgery. Balloon technology was initially cleared by the U.S. Food and Drug Administration in 2005 and is an endoscopic, catheter-based system for chronic sinusitis. It uses a balloon over a wire catheter to dilate sinus passageways. The balloon is inflated with the goal of dilating the sinus openings, widening the walls of the sinus passageway and restoring normal drainage.

Maxillary sinus floor augmentation is a surgical procedure which aims to increase the amount of bone in the posterior maxilla, in the area of the premolar and molar teeth, by lifting the lower Schneiderian membrane and placing a bone graft.
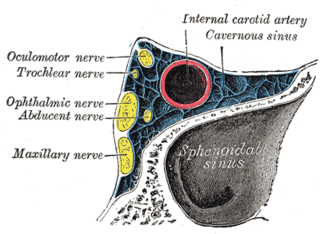
Cavernous sinus thrombosis (CST) is the formation of a blood clot within the cavernous sinus, a cavity at the base of the brain which drains deoxygenated blood from the brain back to the heart. This is a rare disorder and can be of two types–septic cavernous thrombosis and aseptic cavernous thrombosis. The most common form is septic cavernous sinus thrombosis. The cause is usually from a spreading infection in the nose, sinuses, ears, or teeth. Staphylococcus aureus and Streptococcus are often the associated bacteria.

Functional endoscopic sinus surgery (FESS) is a procedure that is used to treat sinusitis and other conditions that affect the sinuses. Sinusitis is an inflammation of the sinuses that can cause symptoms such as congestion, headaches, and difficulty breathing through the nose.

An orbital blowout fracture is a traumatic deformity of the orbital floor or medial wall that typically results from the impact of a blunt object larger than the orbital aperture, or eye socket. Most commonly this results in a herniation of orbital contents through the orbital fractures. The proximity of maxillary and ethmoidal sinus increases the susceptibility of the floor and medial wall for the orbital blowout fracture in these anatomical sites. Most commonly, the inferior orbital wall, or the floor, is likely to collapse, because the bones of the roof and lateral walls are robust. Although the bone forming the medial wall is the thinnest, it is buttressed by the bone separating the ethmoidal air cells. The comparatively thin bone of the floor of the orbit and roof of the maxillary sinus has no support and so the inferior wall collapses mostly. Therefore, medial wall blowout fractures are the second-most common, and superior wall, or roof and lateral wall, blowout fractures are uncommon and rare, respectively. They are characterized by double vision, sunken ocular globes, and loss of sensation of the cheek and upper gums from infraorbital nerve injury.

An odontogenic infection is an infection that originates within a tooth or in the closely surrounding tissues. The term is derived from odonto- and -genic. The most common causes for odontogenic infection to be established are dental caries, deep fillings, failed root canal treatments, periodontal disease, and pericoronitis. Odontogenic infection starts as localised infection and may remain localised to the region where it started, or spread into adjacent or distant areas.

A Sinus implant is a medical device that is inserted into the sinus cavity. Implants can be in conjunction with sinus surgery to treat chronic sinusitis and also in sinus augmentation to increase bone structure for placement of dental implants.
Endoscopic ear surgery (EES) is a minimally invasive alternative to traditional ear surgery and is defined as the use of the rigid endoscope, as opposed to a surgical microscope, to visualize the middle and inner ear during otologic surgery. During endoscopic ear surgery the surgeon holds the endoscope in one hand while working in the ear with the other. To allow this kind of single-handed surgery, different surgical instruments have to be used. Endoscopic visualization has improved due to high-definition video imaging and wide-field endoscopy, and being less invasive, EES is gaining importance as an adjunct to microscopic ear surgery.
Antral lavage is a largely obsolete surgical procedure in which a cannula is inserted into the maxillary sinus via the inferior meatus to allow irrigation and drainage of the sinus. It is also called proof puncture, as the presence of an infection can be proven during the procedure. Upon presence of infection, it can be considered as therapeutic puncture. Often, multiple repeated lavages are subsequently required to allow for full washout of infection.
Caldwell-Luc surgery, Caldwell-Luc operation, also known as Caldwell-Luc antrostomy, and Radical antrostomy, is an operation to remove irreversibly damaged mucosa of the maxillary sinus. It is done when maxillary sinusitis is not cured by medication or other non-invasive technique. The approach is mainly from the anterior wall of the maxilla bone. It was introduced by George Caldwell (1893)and Henry Luc (1897). The maxillary sinus is entered from two separate openings, one in the canine fossa to gain access to the antrum and other in the naso antral wall for drainage.

Oroantral fistula (OAF) is an epithelialised oroantral communication (OAC). OAC refers to an abnormal connection between the oral cavity and antrum. The creation of an OAC is most commonly due to the extraction of a maxillary (upper) tooth closely related to the antral floor. A small OAC may heal spontaneously but a larger OAC would require surgical closure to prevent the development of persistent OAF and chronic sinusitis.
Eustachian tube dysfunction (ETD) is a disorder where pressure abnormalities in the middle ear result in symptoms.
Muaaz Tarabichi is a Syrian otolaryngologist, lecturer, researcher, and author. He is recognized around the world as the father of endoscopic ear surgery. He is the co-founder of Tarabichi Stammberger Ear and Sinus Institute. He was elected as the chairman of the International Advisory Board of the American Academy of Otolaryngology–Head and Neck Surgery.

Orbital emphysema is a medical condition that refers to the trapping of air within the loose subcutaneous around the orbit that is generally characterized by sudden onset swelling and bruising at the impacted eye, with or without deterioration of vision, which the severity depends on the density of air trapped under the orbital soft tissue spaces.
Odontogenic sinusitis is a type of sinusitis, specifically caused by dental infections or procedures. Comprising approximately 10-12% of all chronic sinusitis cases, this condition primarily affects the maxillary sinus, which is in close proximity to the upper teeth.
References
- 1 2 3 4 5 6 7 8 9 10 Stryjewska-Makuch, Grażyna; Goroszkiewicz, Karolina; Szymocha, Jerzy; Lisowska, Grażyna; Misiołek, Maciej (3 September 2021). "Etiology, Early Diagnosis and Proper Treatment of Silent Sinus Syndrome Based on Review of the Literature and Own Experience". Journal of Oral and Maxillofacial Surgery . 80 (1): 113.e1–113.e8. doi: 10.1016/j.joms.2021.08.166 . ISSN 0278-2391. PMID 34597532. S2CID 238249024.
- 1 2 3 Annino, Donald J. Jr; Goguen, Laura A. (February 2008). "Silent sinus syndrome". Current Opinion in Otolaryngology & Head and Neck Surgery. 16 (1): 22–25. doi:10.1097/MOO.0b013e3282f2c9aa. ISSN 1068-9508. PMID 18197017. S2CID 35744217.
- ↑ Sivrice, M.; Yasan, H.; Okur, N.; Okur, E.; Buyukcelik, B.; Kumbul, Y. (10 Jan 2022). "Prevalence of chronic maxillary atelectasis: A radiological study". Journal of Laryngology & Otology. 136 (12): 1240–1244. doi: 10.1017/S0022215122000056 . PMID 35000660. S2CID 253512002 . Retrieved 20 Apr 2022.
- 1 2 Ho, J.; Wong, E.; Gunaratne, D.; Singh, N. (18 Feb 2019). "Chronic maxillary atelectasis (including silent sinus syndrome) can present bilaterally". Journal of Laryngology & Otology. 133 (3): 251–255. doi:10.1017/S0022215119000252. PMID 30773158. S2CID 73497631 . Retrieved 20 Apr 2022.
- ↑ de Dorlodot, C.; Collet, S.; Rombaux, P.; Horoi, M.; Hassid, S.; Eloy, P. (2017). "Chronic maxillary atelectasis and silent sinus syndrome: two faces of the same clinical entity". Eur Arch Otorhinolaryngol. 274 (9): 3367–73. doi:10.1007/s00405-017-4622-8. PMID 28573375. S2CID 7917436.
- ↑ Albadr, Fahad B. (2020). "Silent Sinus Syndrome: Interesting Computed Tomography and Magnetic Resonance Imaging Findings". Journal of Clinical Imaging Science. 10: 38. doi:10.25259/JCIS_62_2020. PMC 7332466 . PMID 32637229.
- ↑ Hlaváčová, Radka; Kuběna, Tomáš; Černošek, Pavel (2019). "Silent sinus syndrome". Czech and Slovak Ophthalmology. 74 (6): 245–248. doi: 10.31348/2018/6/5 . PMID 31238693. S2CID 192493349.
- ↑ Kikuta, Shu; Horikiri, Kyohei; Kanaya, Kaori; Kagoya, Ryoji; Kondo, Kenji; Yamasoba, Tatsuya (2017). "Repetitive Sinus-Related Symptoms May Accelerate the Progression of Chronic Maxillary Atelectasis". Case Reports in Otolaryngology. 2017: 1–5. doi: 10.1155/2017/4296195 . PMC 5512096 . PMID 28758040.
- ↑ Mangussi-Gomes, João; Nakanishi, Márcio; Chalita, Maria Regina; Damasco, Fabiana; Oliveira, Carlos Augusto Costa Pires (2013). "Stage II Chronic Maxillary Atelectasis Associated with Subclinical Visual Field Defect". International Archives of Otorhinolaryngology. 17 (4): 409–412. doi:10.1055/s-0033-1351679. PMC 4399176 . PMID 25992047.
- ↑ George, Jonathan; Durr, Megan; Pletcher, Steven (2011). "Endoscopic Treatment of Silent Sinus Syndrome with Dramatic Resolution". The Laryngoscope. 121: S230. doi:10.1002/lary.22116. S2CID 71631041.
- ↑ Hunt, Scott M; Tami, Thomas A (August 2000). "Sinusitis-induced enophthalmos: The sllent sinus syndrome". Ear, Nose & Throat Journal. 79 (8): 576–584. doi: 10.1177/014556130007900810 . S2CID 44310054.
- ↑ Gunaratne, Dakshika A.; Hasan, Zubair; Floros, Peter; Singh, Narinder (2016). "Bilateral stage I chronic maxillary atelectasis: a case report". Int J Surg Case Rep. 26: 53–6. doi:10.1016/j.ijscr.2016.07.014. PMC 4961494 . PMID 27451129.
- ↑ Arnon, R; Gluck, O; Winter, H; Pikkel, J; Rubinov, A (2019). "Combined Single-Step Procedure for Correction of Silent Sinus Syndrome". Case Rep Ophthalmol. 10 (1): 95–100. doi:10.1159/000498964. PMC 6489024 . PMID 31097950.
- ↑ Cardesín, Alda; Escamilla, Yolanda; Romera, Manuel; Molina, Juan Antonio (2013). "Single Surgical Step for Endoscopic Surgery and Orbital Reconstruction of a Silent Sinus Syndrome". Acta Otorrinolaringologica (English Edition). 64 (4): 297–299. doi:10.1016/j.otoeng.2013.08.010. ISSN 2173-5735. PMID 22421390.
- ↑ Sesenna, Enrico; Oretti, Gabriele; Anghinoni, Marilena Laura; Ferri, Andrea (2010). "Simultaneous management of the enophthalmos and sinus pathology in silent sinus syndrome: A report of three cases". Journal of Cranio-Maxillofacial Surgery. 38 (6): 469–472. doi:10.1016/j.jcms.2009.12.003. PMID 20096597.
- ↑ Sivasubramaniam, R; Sacks, R; Thornton, M (2011). "Silent sinus syndrome: dynamic changes in the position of the orbital floor after restoration of normal sinus pressure". Journal of Laryngology & Otology. 125 (12): 1239–1243. doi: 10.1017/S0022215111001952 . PMID 21835074. S2CID 23539528.
- ↑ Babar-Craigh, H.; Kayhanian, H.; De Silva D.J.; Rose, G.E.; Lund, V.J. (2011). "Spontaneous silent sinus syndrome (imploding antrum syndrome): Case series of 16 patients". Rhinology. 49 (3): 315–317. doi: 10.4193/Rhino10.103 . PMID 21858262.
- ↑ Thomas, Robert; Graham, Scott; Carter, Keith; Nerad, Jeffrey (Mar 2003). "Management of the Orbital Floor in Silent Sinus Syndrome". American Journal of Rhinology. 17 (2): 97–100. doi:10.1177/194589240301700206. PMID 12751704. S2CID 24006400.
Bibliography
- Illner A, Davidson HC, Harnsberger HR, Hoffman J (2002). "The silent sinus syndrome: clinical and radiographic findings". AJR Am J Roentgenol. 178 (2): 503–6. doi:10.2214/ajr.178.2.1780503. PMID 11804926. Full text
- Numa WA, Desai U, Gold DR, Heher KL, Annino DJ (2005). "Silent sinus syndrome: a case presentation and comprehensive review of all 84 reported cases". Ann Otol Rhinol Laryngol. 114 (9): 688–94. doi:10.1177/000348940511400906. PMID 16240931. S2CID 19348879.
- Habicht ME, Eppenberger PE, Galassi FM, Rühli FJ, Henneberg M (2018). "Queen Meresankh III – the oldest case of bilateral Silent Sinus Syndrome (c. 2620/10 - 2570 BC)?". Anthropologie. 56 (2): 103–113. doi:10.26720/anthro.17.09.25.2.