Bipolar I disorder is a type of bipolar spectrum disorder characterized by the occurrence of at least one manic episode, with or without mixed or psychotic features. Most people also, at other times, have one or more depressive episodes. Typically, these manic episodes can last at least 7 days for most of each day to the extent that the individual may need medical attention. Also, the depressive episodes will be approximately 2 weeks long.

The Diagnostic and Statistical Manual of Mental Disorders is a publication by the American Psychiatric Association (APA) for the classification of mental disorders using a common language and standard criteria. It is the main book for the diagnosis and treatment of mental disorders in the United States and Australia, while in other countries it may be used in conjunction with other documents. The DSM-5 is considered one of the principal guides of psychiatry, along with the International Classification of Diseases (ICD), Chinese Classification of Mental Disorders (CCMD), and the Psychodynamic Diagnostic Manual. However, not all providers rely on the DSM-5 as a guide, since the ICD's mental disorder diagnoses are used around the world and scientific studies often measure changes in symptom scale scores rather than changes in DSM-5 criteria to determine the real-world effects of mental health interventions.
Schizoaffective disorder is a mental disorder characterized by abnormal thought processes and an unstable mood. This diagnosis requires symptoms of both schizophrenia and a mood disorder: either bipolar disorder or depression. The main criterion is the presence of psychotic symptoms for at least two weeks without any mood symptoms. Schizoaffective disorder can often be misdiagnosed when the correct diagnosis may be psychotic depression, bipolar I disorder, schizophreniform disorder, or schizophrenia. This is a problem as treatment and prognosis differ greatly for most of these diagnoses.

A thought disorder (TD) is a disturbance in cognition which affects language, thought and communication. Psychiatric and psychological glossaries in 2015 and 2017 identified thought disorders as encompassing poverty of ideas, neologisms, paralogia, word salad, and delusions—all disturbances of thought content and form. Two specific terms have been suggested—content thought disorder (CTD) and formal thought disorder (FTD). CTD has been defined as a thought disturbance characterized by multiple fragmented delusions, and the term thought disorder is often used to refer to an FTD: a disruption of the form of thought. Also known as disorganized thinking, FTD results in disorganized speech and is recognized as a major feature of schizophrenia and other psychoses. Disorganized speech leads to an inference of disorganized thought. Thought disorders include derailment, pressured speech, poverty of speech, tangentiality, verbigeration, and thought blocking. One of the first known cases of thought disorders, or specifically OCD as it is known today, was in 1691. John Moore, who was a bishop, had a speech in front of Queen Mary II, about "religious melancholy."

A mood swing is an extreme or sudden change of mood. Such changes can play a positive part in promoting problem solving and in producing flexible forward planning, or be disruptive. When mood swings are severe, they may be categorized as part of a mental illness, such as bipolar disorder, where erratic and disruptive mood swings are a defining feature.
Dysphoria is a profound state of unease or dissatisfaction. It is the semantic opposite of euphoria. In a psychiatric context, dysphoria may accompany depression, anxiety, or agitation.
Thought broadcasting is a type of delusional condition in which the affected person believes that others can hear their inner thoughts, despite a clear lack of evidence. The person may believe that either those nearby can perceive their thoughts or that they are being transmitted via mediums such as television, radio or the internet. Different people can experience thought broadcasting in different ways. Thought broadcasting is most commonly found among people who have a psychotic disorder, specifically schizophrenia.
Multiple complex developmental disorder (MCDD) is a research category, proposed to involve several neurological and psychological symptoms where at least some symptoms are first noticed during early childhood and persist throughout life. It was originally suggested to be a subtype of pervasive developmental disorders (PDD) with co-morbid schizophrenia or another psychotic disorder; however, there is some controversy that not everyone with MCDD meets criteria for both PDD and psychosis. The term multiplex developmental disorder was coined by Donald J. Cohen in 1986.
The classification of mental disorders, also known as psychiatric nosology or psychiatric taxonomy, is central to the practice of psychiatry and other mental health professions.

The Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5), is the 2013 update to the Diagnostic and Statistical Manual of Mental Disorders, the taxonomic and diagnostic tool published by the American Psychiatric Association (APA). In 2022, a revised version (DSM-5-TR) was published. In the United States, the DSM serves as the principal authority for psychiatric diagnoses. Treatment recommendations, as well as payment by health care providers, are often determined by DSM classifications, so the appearance of a new version has practical importance. However, not all providers rely on the DSM-5 for planning treatment as the ICD's mental disorder diagnoses are used around the world and scientific studies often measure changes in symptom scale scores rather than changes in DSM-5 criteria to determine the real-world effects of mental health interventions. The DSM-5 is the only DSM to use an Arabic numeral instead of a Roman numeral in its title, as well as the only living document version of a DSM.
Personality disorders (PD) are a class of mental disorders characterized by enduring maladaptive patterns of behavior, cognition, and inner experience, exhibited across many contexts and deviating from those accepted by the individual's culture. These patterns develop early, are inflexible, and are associated with significant distress or disability. The definitions vary by source and remain a matter of controversy. Official criteria for diagnosing personality disorders are listed in the sixth chapter of the International Classification of Diseases (ICD) and in the American Psychiatric Association's Diagnostic and Statistical Manual of Mental Disorders (DSM).
Cyclothymia, also known as cyclothymic disorder, psychothemia / psychothymia, bipolar III, affective personality disorder and cyclothymic personality disorder, is a mental and behavioural disorder that involves numerous periods of symptoms of depression and periods of symptoms of elevated mood. These symptoms, however, are not sufficient to indicate a major depressive episode or a manic episode. Symptoms must last for more than one year in children and two years in adults.
Childhood schizophrenia is similar in characteristics of schizophrenia that develops at a later age, but has an onset before the age of 13 years, and is more difficult to diagnose. Schizophrenia is characterized by positive symptoms that can include hallucinations, delusions, and disorganized speech; negative symptoms, such as blunted affect and avolition and apathy, and a number of cognitive impairments. Differential diagnosis is problematic since several other neurodevelopmental disorders, including autism spectrum disorder, language disorder, and attention deficit hyperactivity disorder, also have signs and symptoms similar to childhood-onset schizophrenia.
The diagnosis of schizophrenia, a psychotic disorder, is based on criteria in either the American Psychiatric Association's Diagnostic and Statistical Manual of Mental Disorders, or the World Health Organization's International Classification of Diseases (ICD). Clinical assessment of schizophrenia is carried out by a mental health professional based on observed behavior, reported experiences, and reports of others familiar with the person. Diagnosis is usually made by a psychiatrist. Associated symptoms occur along a continuum in the population and must reach a certain severity and level of impairment before a diagnosis is made. Schizophrenia has a prevalence rate of 0.3-0.7% in the United States.
Pseudoneurotic schizophrenia is a postulated mental disorder categorized by the presence of two or more symptoms of mental illness such as anxiety, hysteria, and phobic or obsessive-compulsive neuroses. It is often acknowledged as a personality disorder. Patients generally display salient anxiety symptoms that disguise an underlying psychotic disorder.
Simple-type schizophrenia is a sub-type of schizophrenia included in the International Classification of Diseases (ICD-10), in which it is classified as a mental and behaviour disorder. It is not included in the current Diagnostic and Statistical Manual of Mental Disorders (DSM-5) or the upcoming ICD-11, effective 1 January 2022. Simple-type schizophrenia is characterized by negative ("deficit") symptoms, such as avolition, apathy, anhedonia, reduced affect display, lack of initiative, lack of motivation, low activity; with absence of hallucinations or delusions of any kind.
The Kiddie Schedule for Affective Disorders and Schizophrenia (K-SADS) is a semi-structured interview aimed at early diagnosis of affective disorders such as depression, bipolar disorder, and anxiety disorder. There are different versions of the test that have use different versions of diagnostic criteria, cover somewhat different diagnoses and use different rating scales for the items. All versions are structured to include interviews with both the child and the parents or guardians, and all use a combination of screening questions and more comprehensive modules to balance interview length and thoroughness.
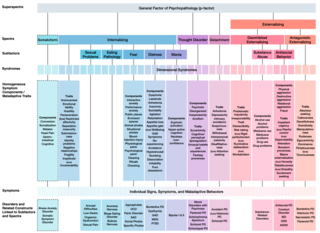
The Hierarchical Taxonomy Of Psychopathology (HiTOP) consortium was formed in 2015 as a grassroots effort to articulate a classification of mental health problems based on recent scientific findings on how the components of mental disorders fit together. The consortium is developing the HiTOP model, a classification system, or taxonomy, of mental disorders, or psychopathology, aiming to prioritize scientific results over convention and clinical opinion. The motives for proposing this classification were to aid clinical practice and mental health research. The consortium was organized by Drs. Roman Kotov, Robert Krueger, and David Watson. At inception it included 40 psychologists and psychiatrists, who had a record of scientific contributions to classification of psychopathology The HiTOP model aims to address limitations of traditional classification systems for mental illness, such as the DSM-5 and ICD-10, by organizing psychopathology according to evidence from research on observable patterns of mental health problems.
