
Cognitive behavioral therapy (CBT) is a psycho-social intervention that aims to reduce symptoms of various mental health conditions, primarily depression and anxiety disorders. Cognitive behavioral therapy is one of the most effective means of treatment for substance abuse and co-occurring mental health disorders. CBT focuses on challenging and changing cognitive distortions and their associated behaviors to improve emotional regulation and develop personal coping strategies that target solving current problems. Though it was originally designed to treat depression, its uses have been expanded to include the treatment of many mental health conditions, including anxiety, substance use disorders, marital problems, ADHD, and eating disorders. CBT includes a number of cognitive or behavioral psychotherapies that treat defined psychopathologies using evidence-based techniques and strategies.
Twelve-step programs are international mutual aid programs supporting recovery from substance addictions, behavioral addictions and compulsions. Developed in the 1930s, the first twelve-step program, Alcoholics Anonymous (AA), founded by Bill Wilson and Bob Smith, aided its membership to overcome alcoholism. Since that time dozens of other organizations have been derived from AA's approach to address problems as varied as drug addiction, compulsive gambling, sex, and overeating. All twelve-step programs utilize a version of AA's suggested twelve steps first published in the 1939 book Alcoholics Anonymous: The Story of How More Than One Hundred Men Have Recovered from Alcoholism.
Rational Recovery was a commercial vendor of material related to counseling, guidance, and direct instruction for addiction designed as a direct counterpoint to Alcoholics Anonymous (AA) and twelve-step programs.
Drug rehabilitation is the process of medical or psychotherapeutic treatment for dependency on psychoactive substances such as alcohol, prescription drugs, and street drugs such as cannabis, cocaine, heroin or amphetamines. The general intent is to enable the patient to confront substance dependence, if present, and stop substance misuse to avoid the psychological, legal, financial, social, and physical consequences that can be caused.

Anger management is a psycho-therapeutic program for anger prevention and control. It has been described as deploying anger successfully. Anger is frequently a result of frustration, or of feeling blocked or thwarted from something the subject feels is important. Anger can also be a defensive response to underlying fear or feelings of vulnerability or powerlessness. Anger management programs consider anger to be a motivation caused by an identifiable reason which can be logically analyzed and addressed.
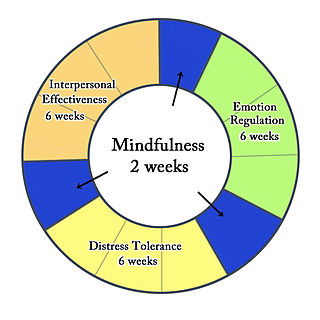
Dialectical behavior therapy (DBT) is an evidence-based psychotherapy that began with efforts to treat personality disorders and interpersonal conflicts. Evidence suggests that DBT can be useful in treating mood disorders and suicidal ideation, as well as for changing behavioral patterns such as self-harm and substance use. DBT evolved into a process in which the therapist and client work with acceptance and change-oriented strategies, and ultimately balance and synthesize them—comparable to the philosophical dialectical process of thesis and antithesis followed by synthesis.
Impulse-control disorder (ICD) is a class of psychiatric disorders characterized by impulsivity – failure to resist a temptation, an urge, or an impulse; or having the inability to not speak on a thought. Many psychiatric disorders feature impulsivity, including substance-related disorders, behavioral addictions, attention deficit hyperactivity disorder, fetal alcohol spectrum disorders, antisocial personality disorder, borderline personality disorder, conduct disorder and some mood disorders.
Substance dependence, also known as drug dependence, is a biopsychological situation whereby an individual's functionality is dependent on the necessitated re-consumption of a psychoactive substance because of an adaptive state that has developed within the individual from psychoactive substance consumption that results in the experience of withdrawal and that necessitates the re-consumption of the drug. A drug addiction, a distinct concept from substance dependence, is defined as compulsive, out-of-control drug use, despite negative consequences. An addictive drug is a drug which is both rewarding and reinforcing. ΔFosB, a gene transcription factor, is now known to be a critical component and common factor in the development of virtually all forms of behavioral and drug addictions, but not dependence.
Contingency management (CM) is the application of the three-term contingency, which uses stimulus control and consequences to change behavior. CM originally derived from the science of applied behavior analysis (ABA), but it is sometimes implemented from a cognitive-behavior therapy (CBT) framework as well.
Motivational therapy is a combination of humanistic treatment and enhanced cognitive-behavioral strategies, designed to treat substance use disorders. It is similar to motivational interviewing and motivational enhancement therapy.
Cognitive therapy (CT) is a type of psychotherapy developed by American psychiatrist Aaron T. Beck. CT is one therapeutic approach within the larger group of cognitive behavioral therapies (CBT) and was first expounded by Beck in the 1960s. Cognitive therapy is based on the cognitive model, which states that thoughts, feelings and behavior are all connected, and that individuals can move toward overcoming difficulties and meeting their goals by identifying and changing unhelpful or inaccurate thinking, problematic behavior, and distressing emotional responses. This involves the individual working with the therapist to develop skills for testing and changing beliefs, identifying distorted thinking, relating to others in different ways, and changing behaviors. A cognitive case conceptualization is developed by the cognitive therapist as a guide to understand the individual's internal reality, select appropriate interventions and identify areas of distress.
Drug addiction recovery groups are voluntary associations of people who share a common desire to overcome their drug addiction. Different groups use different methods, ranging from completely secular to explicitly spiritual. Some programs may advocate a reduction in the use of drugs rather than outright abstention. One survey of members who found active involvement in any addiction recovery group correlates with higher chances of maintaining sobriety. Although there is not a difference in whether group or individual therapy is better for the patient, studies show that any therapy increases positive outcomes for patients with substance use disorder. The survey found group participation increased when the individual members' beliefs matched those of their primary support group. Analysis of the survey results found a significant positive correlation between the religiosity of members and their participation in twelve-step programs and to a lesser level in non-religious SMART Recovery groups, the correlation factor being three times smaller for SMART Recovery than for the twelve-step addiction recovery groups. Religiosity was inversely related to participation in Secular Organizations for Sobriety.
Transference focused psychotherapy (TFP) is a highly structured, twice-weekly modified psychodynamic treatment based on Otto F. Kernberg's object relations model of borderline personality disorder. It views the individual with borderline personality organization (BPO) as holding unreconciled and contradictory internalized representations of self and significant others that are affectively charged. The defense against these contradictory internalized object relations leads to disturbed relationships with others and with self. The distorted perceptions of self, others, and associated affects are the focus of treatment as they emerge in the relationship with the therapist (transference). The treatment focuses on the integration of split off parts of self and object representations, and the consistent interpretation of these distorted perceptions is considered the mechanism of change.
The mainstay of management of borderline personality disorder is various forms of psychotherapy with medications being found to be of little use.
Schema therapy was developed by Jeffrey E. Young for use in treatment of personality disorders and chronic DSM Axis I disorders, such as when patients fail to respond or relapse after having been through other therapies. Schema therapy is an integrative psychotherapy combining theory and techniques from previously existing therapies, including cognitive behavioral therapy, psychoanalytic object relations theory, attachment theory, and Gestalt therapy.

Addiction is generally a neuropsychological disorder defining pervasive and intense urge to engage in maladaptive behaviors providing immediate sensory rewards, despite their harmful consequences. Dependence is generally an addiction that can involve withdrawal issues. Addictive disorder is a category of mental disorders defining important intensities of addictions or dependences, which induce functional disabilities. There are no agreed definitions on these terms – see section on 'definitions'.
About 1 in 7 Americans suffer from active addiction to a particular substance. Addiction can cause physical, psychological, and emotional harm to those who are affected by it. The American Society of Addiction Medicine defines addiction as "a treatable, chronic medical disease involving complex interactions among brain circuits, genetics, the environment, and an individual's life experiences. People with addiction use substances or engage in behaviors that become compulsive and often continue despite harmful consequences." In the world of psychology and medicine, there are two models that are commonly used in understanding the psychology behind addiction itself. One model is referred to as the disease model of addiction. The disease model suggests that addiction is a diagnosable disease similar to cancer or diabetes. This model attributes addiction to a chemical imbalance in an individual's brain that could be caused by genetics or environmental factors. The second model is the choice model of addiction, which holds that addiction is a result of voluntary actions rather than some dysfunction of the brain. Through this model, addiction is viewed as a choice and is studied through components of the brain such as reward, stress, and memory. Substance addictions relate to drugs, alcohol, and smoking. Process addictions relate to non-substance-related behaviors such as gambling, spending money, sexual activity, gaming, spending time on the internet, and eating.
Community reinforcement approach and family training (CRAFT) is a behavior therapy approach in psychotherapy for treating addiction developed by Robert J. Meyers in the late 1970s. Meyers worked with Nathan Azrin in the early 1970s whilst he was developing his own community reinforcement approach (CRA) which uses operant conditioning techniques to help people learn to reduce the power of their addictions and enjoy healthy living. Meyers adapted CRA to create CRAFT, which he described as CRA that "works through family members." CRAFT combines CRA with family training to equip concerned significant others (CSOs) of addicts with supportive techniques to encourage their loved ones to begin and continue treatment and provides them with defences against addiction's damaging effects on themselves.

Robert L. Leahy is a psychologist and author and editor of 29 books dedicated to cognitive behaviour therapy. He is Director of the American Institute for Cognitive Therapy in New York and Clinical Professor of Psychology in the Department of Psychiatry at Weill Cornell Medical College.