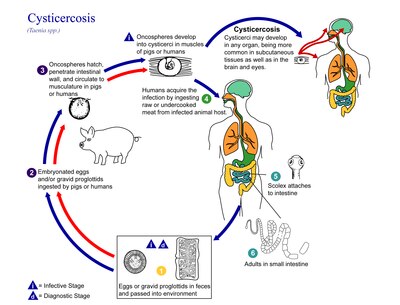
Cysticercosis is a tissue infection caused by the young form of the pork tapeworm. People may have few or no symptoms for years. In some cases, particularly in Asia, solid lumps of between one and two centimetres may develop under the skin. After months or years these lumps can become painful and swollen and then resolve. A specific form called neurocysticercosis, which affects the brain, can cause neurological symptoms. In developing countries this is one of the most common causes of seizures.

Taenia is the type genus of the Taeniidae family of tapeworms. It includes some important parasites of livestock. Members of the genus are responsible for taeniasis and cysticercosis in humans, which are types of helminthiasis belonging to the group of neglected tropical diseases. More than 100 species are recorded. They are morphologically characterized by a ribbon-like body composed of a series of segments called proglottids; hence the name Taenia. The anterior end of the body is the scolex. Some members of the genus Taenia have an armed scolex ; of the two major human parasites, Taenia saginata has an unarmed scolex, while Taenia solium has an armed scolex.
Taenia saginata, commonly known as the beef tapeworm, is a zoonotic tapeworm belonging to the order Cyclophyllidea and genus Taenia. It is an intestinal parasite in humans causing taeniasis and cysticercosis in cattle. Cattle are the intermediate hosts, where larval development occurs, while humans are definitive hosts harbouring the adult worms. It is found globally and most prevalently where cattle are raised and beef is consumed. It is relatively common in Africa, Europe, Southeast Asia, South Asia, and Latin America. Humans are generally infected as a result of eating raw or undercooked beef which contains the infective larvae, called cysticerci. As hermaphrodites, each body segment called proglottid has complete sets of both male and female reproductive systems. Thus, reproduction is by self-fertilisation. From humans, embryonated eggs, called oncospheres, are released with faeces and are transmitted to cattle through contaminated fodder. Oncospheres develop inside muscle, liver, and lungs of cattle into infective cysticerci.

Dwarf tapeworm is a cosmopolitan species though most common in temperate zones, and is one of the most common cestodes infecting humans, especially children.

Taenia crassiceps is a tapeworm in the family Taeniidae. It is a parasitic organism whose adult form infects the intestine of carnivores, like canids. It is related to Taenia solium, the pork tapeworm, and to Taenia saginata, the beef tapeworm. It is commonly found in the Northern Hemisphere, especially throughout Canada and the northern United States.

The Taeniidae are a family of tapeworms. It is the largest family representing the order Cyclophyllidea. It includes many species of medical and veterinary importance, as Taenia solium, Taenia saginata, and Echinococcus granulosus. The Taeniidae are parasites of mammals and many are infectious to humans.

Taenia pisiformis, commonly called the rabbit tapeworm, is an endoparasitic tapeworm which causes infection in lagomorphs, rodents, and carnivores. Adult T. pisiformis typically occur within the small intestines of the definitive hosts, the carnivores. Lagomorphs, the intermediate hosts, are infected by fecal contamination of grasses and other food sources by the definitive hosts. The larval stage is often referred to as Cysticercus pisiformis and is found on the livers and peritoneal cavities of the intermediate hosts. T. pisiformis can be found worldwide.

Taeniasis is an infection within the intestines by adult tapeworms belonging to the genus Taenia. There are generally no or only mild symptoms. Symptoms may occasionally include weight loss or abdominal pain. Segments of tapeworm may be seen in the stool. Complications of pork tapeworm may include cysticercosis.
Eucestoda, commonly referred to as tapeworms, is the larger of the two subclasses of flatworms in the class Cestoda. Larvae have six posterior hooks on the scolex (head), in contrast to the ten-hooked Cestodaria. All tapeworms are endoparasites of vertebrates, living in the digestive tract or related ducts. Examples are the pork tapeworm with a human definitive host, and pigs as the secondary host, and Moniezia expansa, the definitive hosts of which are ruminants.
Neurocysticercosis is a specific form of the infectious parasitic disease cysticercosis that is caused by the infection with Taenia solium, a tapeworm found in pigs. Neurocysticercosis occurs when cysts formed by the infection take hold within the brain, causing neurologic syndromes such as epileptic seizures. It is a common cause of seizures worldwide. It has been called a "hidden epidemic" and "arguably the most common parasitic disease of the human nervous system". Common symptoms of neurocysticercosis include seizures, headaches, blindness, meningitis, and dementia.
Cestoda is a class of parasitic worms in the flatworm phylum (Platyhelminthes). Most of the species—and the best-known—are those in the subclass Eucestoda; they are ribbon-like worms as adults, known as tapeworms. Their bodies consist of many similar units known as proglottids—essentially packages of eggs which are regularly shed into the environment to infect other organisms. Species of the other subclass, Cestodaria, are mainly fish infecting parasites.

Coenurosis is a parasitic infection that results when humans ingest the eggs of dog tapeworm species Taenia multiceps, T. serialis, T. brauni, or T. glomerata.

Raillietina is a genus of tapeworms that includes helminth parasites of vertebrates, mostly of birds. The genus was named in 1920 in honour of a French veterinarian and helminthologist, Louis-Joseph Alcide Railliet. Of the 37 species recorded under the genus, Raillietina demerariensis, R. asiatica, and R. formsana are the only species reported from humans, while the rest are found in birds. R. echinobothrida, R. tetragona, and R. cesticillus are the most important species in terms of prevalence and pathogenicity among wild and domestic birds.
Taenia asiatica, commonly known as Asian taenia or Asian tapeworm, is a parasitic tapeworm of humans and pigs. It is one of the three species of Taenia infecting humans and causes taeniasis. Discovered only in 1980s from Taiwan and other East Asian countries as an unusual species, it is so notoriously similar to Taenia saginata, the beef tapeworm, that it was for a time regarded as a slightly different strain. But anomaly arose as the tapeworm is not of cattle origin, but of pigs. Morphological details also showed significant variations, such as presence of rostellar hooks, shorter body, and fewer body segments. The scientific name designated was then Asian T. saginata. But the taxonomic consensus turns out to be that it is a unique species. It was in 1993 that two Korean parasitologists, Keeseon S. Eom and Han Jong Rim, provided the biological bases for classifying it into a separate species. The use of mitochondrial genome sequence and molecular phylogeny in the late 2000s established the taxonomic status.
Gottlieb Heinrich Friedrich Küchenmeister was a German physician.
Taenia serialis, also known as a Canid tapeworm, is found within canines such as foxes and dogs. Adult T. serialis are parasites of carnivores, particularly dogs, with herbivorous lagomorph mammals such as rabbits and hares, serving as intermediate hosts. In definitive hosts, T. serialis is acquired by eating tissues from a variety of intermediate hosts. Accidental infection of humans though, can occur when eggs are ingested from food or water contaminated with dog feces and the human then becomes the T. serialis intermediate host.
Raillietina tetragona is a parasitic tapeworm belonging to the class Cestoda. It is a cosmopolitan helminth of the small intestine of pigeon, chicken and guinea fowl, and is found throughout the world.

An oncosphere is the larval form of a tapeworm once it has been ingested by an intermediate host animal. The intermediate host must ingest the tapeworm's eggs either in food or water-- once this has happened, the eggs hatch and develop into oncospheres which will then burrow through the gut wall of the intermediate host in order to access the organs or tissues of that host where they will continue the next stage of their development as cysticerci or bladderworms. The bladderworm is a cyst created by the oncosphere. In order to become an adult tapeworm, a cysticercus must then be consumed by its definitive host and establish itself by anchoring in that host's digestive tract. From there, the worm will grow in length and eventually produce proglottids which will exit the intestinal tract with other waste material and then burst, releasing the worm's eggs and completing the cycle.

Taenia hydatigena is one of the adult forms of the canine and feline tapeworm. This infection has a worldwide geographic distribution. Humans with taeniasis can infect other humans or animal intermediate hosts by eggs and gravid proglottids passed in the feces.

Cysticercus is a scientific name given to the young tapeworms (larvae) belonging to the genus Taenia. It is a small, sac-like vesicle resembling a bladder; hence, it is also known as bladder worm. It is filled with fluid, in which the main body of the larva, called scolex, resides. It normally develops from the eggs, which are ingested by the intermediate hosts, such as pigs and cattle. The tissue infection is called cysticercosis. Inside such hosts, they settle in the muscles. When humans eat raw or undercooked pork or beef that is contaminated with cysticerci, the larvae grow into adult worms inside the intestine. Under certain circumstances, specifically for the pork tapeworm, the eggs can be accidentally eaten by humans through contaminated foodstuffs. In such case, the eggs hatch inside the body, generally moving to muscles as well as inside the brain. Such brain infection can lead to a serious medical condition called neurocysticercosis. This disease is the leading cause of acquired epilepsy.