Hyperthyroidism is the condition that occurs due to excessive production of thyroid hormones by the thyroid gland. Thyrotoxicosis is the condition that occurs due to excessive thyroid hormone of any cause and therefore includes hyperthyroidism. Some, however, use the terms interchangeably. Signs and symptoms vary between people and may include irritability, muscle weakness, sleeping problems, a fast heartbeat, heat intolerance, diarrhea, enlargement of the thyroid, hand tremor, and weight loss. Symptoms are typically less severe in the elderly and during pregnancy. An uncommon but life-threatening complication is thyroid storm in which an event such as an infection results in worsening symptoms such as confusion and a high temperature; this often results in death. The opposite is hypothyroidism, when the thyroid gland does not make enough thyroid hormone.
Hypothyroidism is a disorder of the endocrine system in which the thyroid gland does not produce enough thyroid hormones. It can cause a number of symptoms, such as poor ability to tolerate cold, extreme fatigue, muscle aches, constipation, slow heart rate, depression, and weight gain. Occasionally there may be swelling of the front part of the neck due to goitre. Untreated cases of hypothyroidism during pregnancy can lead to delays in growth and intellectual development in the baby or congenital iodine deficiency syndrome.
Thyroid-stimulating hormone (also known as thyrotropin, thyrotropic hormone, or abbreviated TSH) is a pituitary hormone that stimulates the thyroid gland to produce thyroxine (T4), and then triiodothyronine (T3) which stimulates the metabolism of almost every tissue in the body. It is a glycoprotein hormone produced by thyrotrope cells in the anterior pituitary gland, which regulates the endocrine function of the thyroid.

Hashimoto's thyroiditis, also known as chronic lymphocytic thyroiditis and Hashimoto's disease, is an autoimmune disease in which the thyroid gland is gradually destroyed. A slightly broader term is autoimmune thyroiditis, identical other than that it is also used to describe a similar condition without a goiter.
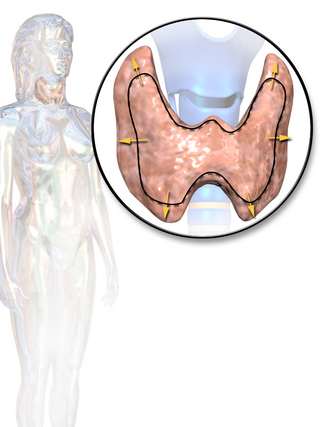
Thyroid disease is a medical condition that affects the function of the thyroid gland. The thyroid gland is located at the front of the neck and produces thyroid hormones that travel through the blood to help regulate many other organs, meaning that it is an endocrine organ. These hormones normally act in the body to regulate energy use, infant development, and childhood development.
Thyroid storm is a rare but severe and life-threatening complication of hyperthyroidism. It occurs when an overactive thyroid leads to hypermetabolism, which can cause death from cardiac arrest or multiple organ failure.

De Quervain's thyroiditis, also known as subacute granulomatous thyroiditis or giant cell thyroiditis, is a member of the group of thyroiditis conditions known as resolving thyroiditis. People of all ages and genders may be affected.
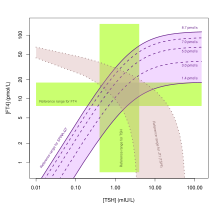
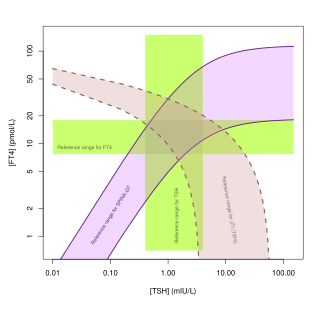
Thyroid function tests (TFTs) is a collective term for blood tests used to check the function of the thyroid. TFTs may be requested if a patient is thought to suffer from hyperthyroidism or hypothyroidism, or to monitor the effectiveness of either thyroid-suppression or hormone replacement therapy. It is also requested routinely in conditions linked to thyroid disease, such as atrial fibrillation and anxiety disorder.

Graves' ophthalmopathy, also known as thyroid eye disease (TED), is an autoimmune inflammatory disorder of the orbit and periorbital tissues, characterized by upper eyelid retraction, lid lag, swelling, redness (erythema), conjunctivitis, and bulging eyes (exophthalmos). It occurs most commonly in individuals with Graves' disease, and less commonly in individuals with Hashimoto's thyroiditis, or in those who are euthyroid.
Postpartum thyroiditis refers to thyroid dysfunction occurring in the first 12 months after pregnancy and may involve hyperthyroidism, hypothyroidism or the two sequentially. According to the National Institute of Health, postpartum thyroiditis affects about 8% of pregnancies. There are, however, different rates reported globally. This is likely due to the differing amounts of average postpartum follow times around the world, and due to humans' own innate differences. For example, in Bangkok, Thailand the rate is 1.1%, but in Brazil it is 13.3%. The first phase is typically hyperthyroidism. Then, the thyroid either returns to normal or a woman develops hypothyroidism. Of those women who experience hypothyroidism associated with postpartum thyroiditis, one in five will develop permanent hypothyroidism requiring lifelong treatment.

The hypothalamic–pituitary–thyroid axis is part of the neuroendocrine system responsible for the regulation of metabolism and also responds to stress.
Hashimoto's encephalopathy, also known as steroid-responsive encephalopathy associated with autoimmune thyroiditis (SREAT), is a neurological condition characterized by encephalopathy, thyroid autoimmunity, and good clinical response to corticosteroids. It is associated with Hashimoto's thyroiditis, and was first described in 1966. It is sometimes referred to as a neuroendocrine disorder, although the condition's relationship to the endocrine system is widely disputed. It is recognized as a rare disease by the NIH Genetic and Rare Diseases Information Center.
Euthyroid sick syndrome (ESS) is a state of adaptation or dysregulation of thyrotropic feedback control wherein the levels of T3 and/or T4 are abnormal, but the thyroid gland does not appear to be dysfunctional. This condition may result from allostatic responses of hypothalamus-pituitary-thyroid feedback control, dyshomeostatic disorders, drug interferences, and impaired assay characteristics in critical illness.
Thyroid disease in pregnancy can affect the health of the mother as well as the child before and after delivery. Thyroid disorders are prevalent in women of child-bearing age and for this reason commonly present as a pre-existing disease in pregnancy, or after childbirth. Uncorrected thyroid dysfunction in pregnancy has adverse effects on fetal and maternal well-being. The deleterious effects of thyroid dysfunction can also extend beyond pregnancy and delivery to affect neurointellectual development in the early life of the child. Due to an increase in thyroxine binding globulin, an increase in placental type 3 deioidinase and the placental transfer of maternal thyroxine to the fetus, the demand for thyroid hormones is increased during pregnancy. The necessary increase in thyroid hormone production is facilitated by high human chorionic gonadotropin (hCG) concentrations, which bind the TSH receptor and stimulate the maternal thyroid to increase maternal thyroid hormone concentrations by roughly 50%. If the necessary increase in thyroid function cannot be met, this may cause a previously unnoticed (mild) thyroid disorder to worsen and become evident as gestational thyroid disease. Currently, there is not enough evidence to suggest that screening for thyroid dysfunction is beneficial, especially since treatment thyroid hormone supplementation may come with a risk of overtreatment. After women give birth, about 5% develop postpartum thyroiditis which can occur up to nine months afterwards. This is characterized by a short period of hyperthyroidism followed by a period of hypothyroidism; 20–40% remain permanently hypothyroid.
Antithyroid autoantibodies (or simply antithyroid antibodies) are autoantibodies targeted against one or more components on the thyroid. The most clinically relevant anti-thyroid autoantibodies are anti-thyroid peroxidase antibodies (anti-TPO antibodies, TPOAb), thyrotropin receptor antibodies (TRAb) and thyroglobulin antibodies (TgAb). TRAb's are subdivided into activating, blocking and neutral antibodies, depending on their effect on the TSH receptor. Anti-sodium/iodide (Anti–Na+/I−) symporter antibodies are a more recent discovery and their clinical relevance is still unknown. Graves' disease and Hashimoto's thyroiditis are commonly associated with the presence of anti-thyroid autoantibodies. Although there is overlap, anti-TPO antibodies are most commonly associated with Hashimoto's thyroiditis and activating TRAb's are most commonly associated with Graves' disease. Thyroid microsomal antibodies were a group of anti-thyroid antibodies; they were renamed after the identification of their target antigen (TPO).
The sum activity of peripheral deiodinases is the maximum amount of triiodothyronine produced per time-unit under conditions of substrate saturation. It is assumed to reflect the activity of deiodinases outside the central nervous system and other isolated compartments. GD is therefore expected to reflect predominantly the activity of type I deiodinase.
Jostel's TSH index, also referred to as Jostel's thyrotropin index or Thyroid Function index (TFI), is a method for estimating the thyrotropic function of the anterior pituitary lobe in a quantitative way. The equation has been derived from the logarithmic standard model of thyroid homeostasis. In a paper from 2014 further study was suggested to show if it is useful, but the 2018 guideline by the European Thyroid Association for the diagnosis of uncertain cases of central hypothyroidism regarded it as beneficial. It is also recommended for purposes of differential diagnosis in the sociomedical expert assessment.

SimThyr is a free continuous dynamic simulation program for the pituitary-thyroid feedback control system. The open-source program is based on a nonlinear model of thyroid homeostasis. In addition to simulations in the time domain the software supports various methods of sensitivity analysis. Its simulation engine is multi-threaded and supports multiple processor cores. SimThyr provides a GUI, which allows for visualising time series, modifying constant structure parameters of the feedback loop, storing parameter sets as XML files and exporting results of simulations in various formats that are suitable for statistical software. SimThyr is intended for both educational purposes and in-silico research.
The Thyrotroph Thyroid Hormone Sensitivity Index is a calculated structure parameter of thyroid homeostasis. It was originally developed to deliver a method for fast screening for resistance to thyroid hormone. Today it is also used to get an estimate for the set point of thyroid homeostasis, especially to assess dynamic thyrotropic adaptation of the anterior pituitary gland, including non-thyroidal illnesses.
The Thyroid Feedback Quantile-based Index (TFQI) is a calculated parameter for thyrotropic pituitary function. It was defined to be more robust to distorted data than established markers including Jostel's TSH index (JTI) and the thyrotroph thyroid hormone sensitivity index (TTSI).