
Cholesteatoma is a destructive and expanding growth consisting of keratinizing squamous epithelium in the middle ear and/or mastoid process. Cholesteatomas are not cancerous as the name may suggest, but can cause significant problems because of their erosive and expansile properties. This can result in the destruction of the bones of the middle ear (ossicles), as well as growth through the base of the skull into the brain. They often become infected and can result in chronically draining ears. Treatment almost always consists of surgical removal.
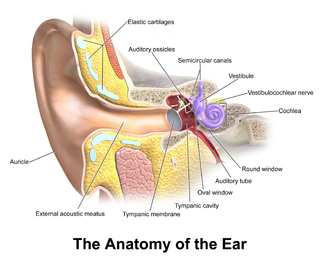
In the anatomy of humans and various other tetrapods, the eardrum, also called the tympanic membrane or myringa, is a thin, cone-shaped membrane that separates the external ear from the middle ear. Its function is to transmit sound from the air to the ossicles inside the middle ear, and then to the oval window in the fluid-filled cochlea. Hence, it ultimately converts and amplifies vibration in the air to vibration in cochlear fluid. The malleus bone bridges the gap between the eardrum and the other ossicles.

Otitis media is a group of inflammatory diseases of the middle ear. One of the two main types is acute otitis media (AOM), an infection of rapid onset that usually presents with ear pain. In young children this may result in pulling at the ear, increased crying, and poor sleep. Decreased eating and a fever may also be present. The other main type is otitis media with effusion (OME), typically not associated with symptoms, although occasionally a feeling of fullness is described; it is defined as the presence of non-infectious fluid in the middle ear which may persist for weeks or months often after an episode of acute otitis media. Chronic suppurative otitis media (CSOM) is middle ear inflammation that results in a perforated tympanic membrane with discharge from the ear for more than six weeks. It may be a complication of acute otitis media. Pain is rarely present. All three types of otitis media may be associated with hearing loss. If children with hearing loss due to OME do not learn sign language, it may affect their ability to learn.

The Eustachian tube, also called the auditory tube or pharyngotympanic tube, is a tube that links the nasopharynx to the middle ear, of which it is also a part. In adult humans, the Eustachian tube is approximately 35 mm (1.4 in) long and 3 mm (0.12 in) in diameter. It is named after the sixteenth-century Italian anatomist Bartolomeo Eustachi.

Otosclerosis is a condition of the middle ear where portions of the dense enchondral layer of the bony labyrinth remodel into one or more lesions of irregularly-laid spongy bone. As the lesions reach the stapes the bone is resorbed, then hardened (sclerotized), which limits its movement and results in hearing loss, tinnitus, vertigo or a combination of symptoms. The term otosclerosis is something of a misnomer: much of the clinical course is characterized by lucent rather than sclerotic bony changes, so the disease is also known as otospongiosis.
Stapedectomy is a surgical procedure in which the stapes bone is removed from the middle ear and replaced with a prosthesis.

Conductive hearing loss (CHL) occurs when there is a problem transferring sound waves anywhere along the pathway through the outer ear, tympanic membrane (eardrum), or middle ear (ossicles). If a conductive hearing loss occurs in conjunction with a sensorineural hearing loss, it is referred to as a mixed hearing loss. Depending upon the severity and nature of the conductive loss, this type of hearing impairment can often be treated with surgical intervention or pharmaceuticals to partially or, in some cases, fully restore hearing acuity to within normal range. However, cases of permanent or chronic conductive hearing loss may require other treatment modalities such as hearing aid devices to improve detection of sound and speech perception.
A myringotomy is a surgical procedure in which an incision is created in the eardrum to relieve pressure caused by excessive buildup of fluid, or to drain pus from the middle ear. A tympanostomy tube may be inserted through the eardrum to keep the middle ear aerated for a prolonged time and to prevent reaccumulation of fluid. Without the insertion of a tube, the incision usually heals spontaneously within two to three weeks. Depending on the type, the tube is either naturally extruded in 6 to 12 months or removed during a minor procedure.

Tympanoplasty is the surgical operation performed to reconstruct hearing mechanism of middle ear.

Otology is a branch of medicine which studies normal and pathological anatomy and physiology of the ear as well as their diseases, diagnosis and treatment. Otologic surgery generally refers to surgery of the middle ear and mastoid related to chronic otitis media, such as tympanoplasty, or ear drum surgery, ossiculoplasty, or surgery of the hearing bones, and mastoidectomy. Otology also includes surgical treatment of conductive hearing loss, such as stapedectomy surgery for otosclerosis.

Tympanostomy tube, also known as a grommet or myringotomy tube, is a small tube inserted into the eardrum in order to keep the middle ear aerated for a prolonged period of time, and to prevent the accumulation of fluid in the middle ear. The operation to insert the tube involves a myringotomy and is performed under local or general anesthesia. The tube itself is made in a variety of designs. The most commonly used type is shaped like a grommet. When it is necessary to keep the middle ear ventilated for a very long period, a "T"-shaped tube may be used, as these "T-tubes" can stay in place for 2–4 years. Materials used to construct the tube are most often plastics such as silicone or Teflon. Stainless steel tubes exist, but are no longer in frequent use.
Burow's solution is an aqueous solution of aluminium triacetate. It is available in the U.S. as an over-the-counter drug for topical administration, with brand names including Domeboro, Domeboro Otic, Star-Otic, and Borofair. The preparation has astringent and antibacterial properties and may be used to treat a number of skin conditions, including insect bites and stings, rashes caused by poison ivy and poison sumac, swelling, allergies, and bruises. However, its main use is for treatment of otitis, including otomycosis.

A perforated eardrum is a hole in the eardrum. It can be caused by infection, trauma, overpressure, inappropriate ear clearing, and changes in middle ear pressure. An otoscope can be used to view the eardrum to diagnose a perforation. Perforations may heal naturally or require surgery.
Hearing loss with craniofacial syndromes is a common occurrence. Many of these multianomaly disorders involve structural malformations of the outer or middle ear, making a significant hearing loss highly likely.
A mastoidectomy is a procedure performed to remove the mastoid air cells, air bubbles in the skull, near the inner ears. This can be done as part of treatment for mastoiditis, chronic suppurative otitis media or cholesteatoma. In addition, it is sometimes performed as part of other procedures or for access to the middle ear. There are classically 5 different types of mastoidectomy:

Tympanic membrane retraction describes a condition in which a part of the eardrum lies deeper within the ear than its normal position.

An otic polyp is a benign proliferation of chronic inflammatory cells associated with granulation tissue, in response to a longstanding inflammatory process of the middle ear.
Nicholas John Frootko is a retired South African / British Otolaryngologist / Head and Neck Surgeon with a special interest and expertise in Ear Surgery.
Eustachian tube dysfunction (ETD) is a disorder where pressure abnormalities in the middle ear result in symptoms.
A middle ear implant is a hearing device that is surgically implanted into the middle ear. They help people with conductive, sensorineural or mixed hearing loss to hear.

{kind=link}