Health care reform- is for the most part, governmental policy that affects health care delivery in a given place. Health care reform typically attempts to:

Medicare is a national health insurance program in the United States, begun in 1966 under the Social Security Administration (SSA) and now administered by the Centers for Medicare and Medicaid Services (CMS). It provides health insurance for Americans aged 65 and older, younger people with some disability status as determined by the Social Security Administration, as well as people with end stage renal disease and amyotrophic lateral sclerosis.
Health insurance is an insurance that covers the whole or a part of the risk of a person incurring medical expenses, spreading the risk over a large number of persons. By estimating the overall risk of health care and health system expenses over the risk pool, an insurer can develop a routine finance structure, such as a monthly premium or payroll tax, to provide the money to pay for the health care benefits specified in the insurance agreement. The benefit is administered by a central organization such as a government agency, private business, or not-for-profit entity.
Health care in Ireland is two-tier: public and private sectors exist. The public health care system is governed by the Health Act 2004, which established a new body to be responsible for providing health and personal social services to everyone living in Ireland – the Health Service Executive. The new national health service came into being officially on 1 January 2005; however the new structures are currently in the process of being established as the reform programme continues. In addition to the public-sector, there is also a large private healthcare market.
The health care system in Japan provides healthcare services, including screening examinations, prenatal care and infectious disease control, with the patient accepting responsibility for 30% of these costs while the government pays the remaining 70%. Payment for personal medical services is offered by a universal health care insurance system that provides relative equality of access, with fees set by a government committee. All residents of Japan are required by the law to have health insurance coverage. People without insurance from employers can participate in a national health insurance programme, administered by local governments. Patients are free to select physicians or facilities of their choice and cannot be denied coverage. Hospitals, by law, must be run as non-profit and be managed by physicians. For-profit corporations are not allowed to own or operate hospitals. Clinics must be owned and operated by physicians.
The Commonwealth of Massachusetts passed a health care reform law in 2006 with the aim of providing health insurance to nearly all of its residents. The law mandated that nearly every resident of Massachusetts obtain a minimum level of insurance coverage, provided free and subsidized health care insurance for residents earning less than 150% and 300%, respectively, of the federal poverty level (FPL) and mandated employers with more than 10 full-time employees provide healthcare insurance. The law was amended significantly in 2008 and twice in 2010 to make it consistent with the federal Affordable Care Act. Major revisions related to health care industry price controls were passed in August 2012, and the employer mandate was repealed in 2013 in favor of the federal mandate. Because Mitt Romney was the governor of Massachusetts at the time, the law has colloquially been called Romneycare, a reference to the nicknaming of the Patient Protection and Affordable Care Act as "Obamacare".

The Swedish health care system is mainly government-funded and decentralized, although private health care also exists. The health care system in Sweden is financed primarily through taxes levied by county councils and municipalities.
Healthcare reform in the United States has a long history. Reforms have often been proposed but have rarely been accomplished. In 2010, landmark reform was passed through two federal statutes enacted in 2010: the Patient Protection and Affordable Care Act (PPACA), signed March 23, 2010, and the Health Care and Education Reconciliation Act of 2010, which amended the PPACA and became law on March 30, 2010.

Germany has a universal multi-payer health care system paid for by a combination of statutory health insurance and "Private Krankenversicherung".
Healthcare in Finland consists of a highly decentralized three-level publicly funded healthcare system and a much smaller private sector. Although the Ministry of Social Affairs and Health has the highest decision-making authority, the municipalities are responsible for providing healthcare to their residents.
Healthcare in Georgia is provided by a universal health care system under which the state funds medical treatment in a mainly privatized system of medical facilities. In 2013, the enactment of a universal health care program triggered universal coverage of government-sponsored medical care of the population and improving access to health care services. Responsibility for purchasing publicly financed health services lies with the Social Service Agency (SSA).
Healthcare in Denmark is largely provided by the local governments of the five regions, with coordination and regulation by central government, while nursing homes, home care, and school health services are the responsibility of the 98 municipalities. Some specialised hospital services are managed centrally.
Health care in Slovenia is organised primarily through the Health Insurance Institute of Slovenia.
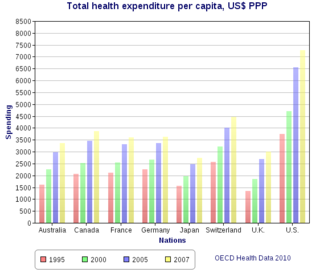
Health care in the United States is provided by many distinct organizations. Health care facilities are largely owned and operated by private sector businesses. 58% of US community hospitals are non-profit, 21% are government owned, and 21% are for-profit. According to the World Health Organization (WHO), the United States spent $9,403 on health care per capita, and 17.1% on health care as percentage of its GDP in 2014. Healthcare coverage is provided through a combination of private health insurance and public health coverage. The United States does not have a universal healthcare program, unlike other advanced industrialized countries.
This article provides a brief overview of the health care systems of the world, sorted by continent.
The elderly population is one of the most vulnerable populations in the world of health care, mainly because of their susceptibility to contracting disease, limited access to health care insurance, limited or non-existent access to long-term care insurance, and/or reduced quality of life. In Germany, the majority of the population, including the elderly is funded by a public health care insurance system. Only employees who have an income above a cutoff point and certain other groups have the option of purchasing private insurance. For the most part, Germany raises money for this health system through statutory welfare contributions.
The Indian Constitution makes the provision of healthcare in India the responsibility of the state governments, rather than the central federal government. It makes every state responsible for "raising the level of nutrition and the standard of living of its people and the improvement of public health as among its primary duties".


