Related Research Articles
In computer science, garbage in, garbage out (GIGO) is the concept that flawed, or nonsense (garbage) input data produces nonsense output. Rubbish in, rubbish out (RIRO) is an alternate wording.

Hearing loss is a partial or total inability to hear. Hearing loss may be present at birth or acquired at any time afterwards. Hearing loss may occur in one or both ears. In children, hearing problems can affect the ability to acquire spoken language, and in adults it can create difficulties with social interaction and at work. Hearing loss can be temporary or permanent. Hearing loss related to age usually affects both ears and is due to cochlear hair cell loss. In some people, particularly older people, hearing loss can result in loneliness. Deaf people usually have little to no hearing.
This is a glossary of medical terms related to communication disorders which are psychological or medical conditions that could have the potential to affect the ways in which individuals can hear, listen, understand, speak and respond to others.
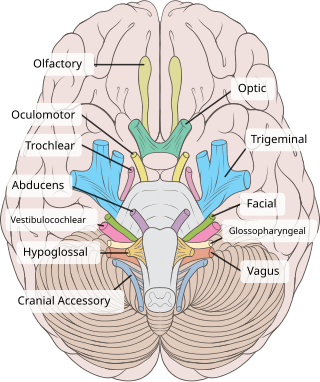
The vestibulocochlear nerve or auditory vestibular nerve, also known as the eighth cranial nerve, cranial nerve VIII, or simply CN VIII, is a cranial nerve that transmits sound and equilibrium (balance) information from the inner ear to the brain. Through olivocochlear fibers, it also transmits motor and modulatory information from the superior olivary complex in the brainstem to the cochlea.

The McGurk effect is a perceptual phenomenon that demonstrates an interaction between hearing and vision in speech perception. The illusion occurs when the auditory component of one sound is paired with the visual component of another sound, leading to the perception of a third sound. The visual information a person gets from seeing a person speak changes the way they hear the sound. If a person is getting poor-quality auditory information but good-quality visual information, they may be more likely to experience the McGurk effect. Integration abilities for audio and visual information may also influence whether a person will experience the effect. People who are better at sensory integration have been shown to be more susceptible to the effect. Many people are affected differently by the McGurk effect based on many factors, including brain damage and other disorders.
Stimulus modality, also called sensory modality, is one aspect of a stimulus or what is perceived after a stimulus. For example, the temperature modality is registered after heat or cold stimulate a receptor. Some sensory modalities include: light, sound, temperature, taste, pressure, and smell. The type and location of the sensory receptor activated by the stimulus plays the primary role in coding the sensation. All sensory modalities work together to heighten stimuli sensation when necessary.

Audiology is a branch of science that studies hearing, balance, and related disorders. Audiologists treat those with hearing loss and proactively prevent related damage. By employing various testing strategies, audiologists aim to determine whether someone has normal sensitivity to sounds. If hearing loss is identified, audiologists determine which portions of hearing are affected, to what degree, and where the lesion causing the hearing loss is found. If an audiologist determines that a hearing loss or vestibular abnormality is present, they will provide recommendations for interventions or rehabilitation.
An otoacoustic emission (OAE) is a sound that is generated from within the inner ear. Having been predicted by Austrian astrophysicist Thomas Gold in 1948, its existence was first demonstrated experimentally by British physicist David Kemp in 1978, and otoacoustic emissions have since been shown to arise through a number of different cellular and mechanical causes within the inner ear. Studies have shown that OAEs disappear after the inner ear has been damaged, so OAEs are often used in the laboratory and the clinic as a measure of inner ear health.

Audiometry is a branch of audiology and the science of measuring hearing acuity for variations in sound intensity and pitch and for tonal purity, involving thresholds and differing frequencies. Typically, audiometric tests determine a subject's hearing levels with the help of an audiometer, but may also measure ability to discriminate between different sound intensities, recognize pitch, or distinguish speech from background noise. Acoustic reflex and otoacoustic emissions may also be measured. Results of audiometric tests are used to diagnose hearing loss or diseases of the ear, and often make use of an audiogram.
Auditory neuropathy (AN) is a hearing disorder in which the outer hair cells of the cochlea are present and functional, but sound information is not transmitted sufficiently by the auditory nerve to the brain. Hearing loss with AN can range from normal hearing sensitivity to profound hearing loss.

Neurofibromatosis type II is a genetic condition that may be inherited or may arise spontaneously, and causes benign tumors of the brain, spinal cord, and peripheral nerves. The types of tumors frequently associated with NF2 include vestibular schwannomas, meningiomas, and ependymomas. The main manifestation of the condition is the development of bilateral benign brain tumors in the nerve sheath of the cranial nerve VIII, which is the "auditory-vestibular nerve" that transmits sensory information from the inner ear to the brain. Besides, other benign brain and spinal tumors occur. Symptoms depend on the presence, localisation and growth of the tumor(s), in which multiple cranial nerves can be involved. Many people with this condition also experience vision problems. Neurofibromatosis type II is caused by mutations of the "Merlin" gene, which seems to influence the form and movement of cells. The principal treatments consist of neurosurgical removal of the tumors and surgical treatment of the eye lesions. Historically the underlying disorder has not had any therapy due to the cell function caused by the genetic mutation.
The auditory brainstem response (ABR), also called brainstem evoked response audiometry (BERA), is an auditory evoked potential extracted from ongoing electrical activity in the brain and recorded via electrodes placed on the scalp. The measured recording is a series of six to seven vertex positive waves of which I through V are evaluated. These waves, labeled with Roman numerals in Jewett and Williston convention, occur in the first 10 milliseconds after onset of an auditory stimulus. The ABR is considered an exogenous response because it is dependent upon external factors.

Cortical deafness is a rare form of sensorineural hearing loss caused by damage to the primary auditory cortex. Cortical deafness is an auditory disorder where the patient is unable to hear sounds but has no apparent damage to the structures of the ear. It has been argued to be as the combination of auditory verbal agnosia and auditory agnosia. Patients with cortical deafness cannot hear any sounds, that is, they are not aware of sounds including non-speech, voices, and speech sounds. Although patients appear and feel completely deaf, they can still exhibit some reflex responses such as turning their head towards a loud sound.
An auditory brainstem implant (ABI) is a surgically implanted electronic device that provides a sense of sound to a person who is profoundly deaf, due to retrocochlear hearing impairment. In Europe, ABIs have been used in children and adults, and in patients with neurofibromatosis type II.

Hearing, or auditory perception, is the ability to perceive sounds through an organ, such as an ear, by detecting vibrations as periodic changes in the pressure of a surrounding medium. The academic field concerned with hearing is auditory science.
Spatial hearing loss refers to a form of deafness that is an inability to use spatial cues about where a sound originates from in space. Poor sound localization in turn affects the ability to understand speech in the presence of background noise.
Amblyaudia is a term coined by Dr. Deborah Moncrieff to characterize a specific pattern of performance from dichotic listening tests. Dichotic listening tests are widely used to assess individuals for binaural integration, a type of auditory processing skill. During the tests, individuals are asked to identify different words presented simultaneously to the two ears. Normal listeners can identify the words fairly well and show a small difference between the two ears with one ear slightly dominant over the other. For the majority of listeners, this small difference is referred to as a "right-ear advantage" because their right ear performs slightly better than their left ear. But some normal individuals produce a "left-ear advantage" during dichotic tests and others perform at equal levels in the two ears. Amblyaudia is diagnosed when the scores from the two ears are significantly different with the individual's dominant ear score much higher than the score in the non-dominant ear Researchers interested in understanding the neurophysiological underpinnings of amblyaudia consider it to be a brain based hearing disorder that may be inherited or that may result from auditory deprivation during critical periods of brain development. Individuals with amblyaudia have normal hearing sensitivity but have difficulty hearing in noisy environments like restaurants or classrooms. Even in quiet environments, individuals with amblyaudia may fail to understand what they are hearing, especially if the information is new or complicated. Amblyaudia can be conceptualized as the auditory analog of the better known central visual disorder amblyopia. The term “lazy ear” has been used to describe amblyaudia although it is currently not known whether it stems from deficits in the auditory periphery or from other parts of the auditory system in the brain, or both. A characteristic of amblyaudia is suppression of activity in the non-dominant auditory pathway by activity in the dominant pathway which may be genetically determined and which could also be exacerbated by conditions throughout early development.
An audiologist, according to the American Academy of Audiology, "is a person who, by virtue of academic degree, clinical training, and license to practice and/or professional credential, is uniquely qualified to provide a comprehensive array of professional services related to the prevention of hearing loss and the audiologic identification, assessment, diagnosis, and treatment of persons with impairment of auditory and vestibular function, and to the prevention of impairments associated with them."
Causes of hearing loss include ageing, genetics, perinatal problems, loud sounds, and diseases. For some kinds of hearing loss the cause may be classified as of unknown cause.

Identification of a hearing loss is usually conducted by a general practitioner medical doctor, otolaryngologist, certified and licensed audiologist, school or industrial audiometrist, or other audiometric technician. Diagnosis of the cause of a hearing loss is carried out by a specialist physician or otorhinolaryngologist.
References
- ↑ Starr, A.; Picton, T.W.; Sininger, Y.; Hood, L.J.; Berlin, C.I. (1996). "Auditory neuropathy". Brain. 119 (3): 741–753. doi: 10.1093/brain/119.3.741 . PMID 8673487.
- ↑ Berlin, C.I.; Hood, L.J.; Rose, K. (2001). "On renaming auditory neuropathy as auditory dys-synchrony" (PDF). Audiology Today. 13: 15–17. Archived from the original (PDF) on 2020-11-24. Retrieved 2020-06-26.
- ↑ Berlin, C.I.; Morlet, T.; Hood, L.J. (2008). "Management of Individuals With Auditory Neuropathy Spectrum Disorder".
{{cite journal}}: Cite journal requires|journal=(help)