Related Research Articles

Metastasis is a pathogenic agent's spread from an initial or primary site to a different or secondary site within the host's body; the term is typically used when referring to metastasis by a cancerous tumor. The newly pathological sites, then, are metastases (mets). It is generally distinguished from cancer invasion, which is the direct extension and penetration by cancer cells into neighboring tissues.

A bone tumor is an abnormal growth of tissue in bone, traditionally classified as noncancerous (benign) or cancerous (malignant). Cancerous bone tumors usually originate from a cancer in another part of the body such as from lung, breast, thyroid, kidney and prostate. There may be a lump, pain, or neurological signs from pressure. A bone tumor might present with a pathologic fracture. Other symptoms may include fatigue, fever, weight loss, anemia and nausea. Sometimes there are no symptoms and the tumour is found when investigating another problem.
In medical or research imaging, an incidental imaging finding is an unanticipated finding which is not related to the original diagnostic inquiry. As with other types of incidental medical findings, they may represent a diagnostic, ethical, and philosophical dilemma because their significance is unclear. While some coincidental findings may lead to beneficial diagnoses, others may lead to overdiagnosis that results in unnecessary testing and treatment, sometimes called the "cascade effect".

A Pancoast tumor is a tumor of the apex of the lung. It is a type of lung cancer defined primarily by its location situated at the top end of either the right or left lung. It typically spreads to nearby tissues such as the ribs and vertebrae. Most Pancoast tumors are non-small-cell lung cancers.

A chest radiograph, chest X-ray (CXR), or chest film is a projection radiograph of the chest used to diagnose conditions affecting the chest, its contents, and nearby structures. Chest radiographs are the most common film taken in medicine.

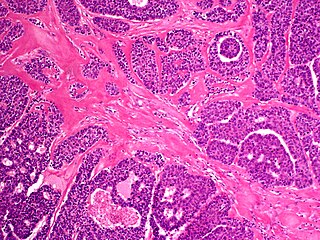
Papillary thyroid cancer is the most common type of thyroid cancer, representing 75 percent to 85 percent of all thyroid cancer cases. It occurs more frequently in women and presents in the 20–55 year age group. It is also the predominant cancer type in children with thyroid cancer, and in patients with thyroid cancer who have had previous radiation to the head and neck. It is often well-differentiated, slow-growing, and localized, although it can metastasize.
Carcinosis, or carcinomatosis, is disseminated cancer, forms of metastasis, whether used generally or in specific patterns of spread.

A lung nodule or pulmonary nodule is a relatively small focal density in the lung. A solitary pulmonary nodule (SPN) or coin lesion, is a mass in the lung smaller than three centimeters in diameter. A pulmonary micronodule has a diameter of less than three millimetres. There may also be multiple nodules.
Malignant acrospiroma, also known as nodular hidradenocarcinoma, malignant nodular clear-cell hidradenoma, mucoepidermoid hidradenocarcinoma, clear-cell hidradenocarcinoma, malignant clear-cell acrospiroma, and clear-cell eccrine carcinoma, is a rare and aggressive tumour of the eccrine sweat glands. It was first documented by Keasbey and Hadley in 1954.

Bone metastasis, or osseous metastatic disease, is a category of cancer metastases that result from primary tumor invasions into bones. Bone-originating primary tumors such as osteosarcoma, chondrosarcoma, and Ewing sarcoma are rare; the most common bone tumor is a metastasis. Bone metastases can be classified as osteolytic, osteoblastic, or both. Unlike hematologic malignancies which originate in the blood and form non-solid tumors, bone metastases generally arise from epithelial tumors and form a solid mass inside the bone. Primary breast cancer patients are particularly vulnerable to develop bone metastases. Bone metastases, especially in a state of advanced disease, can cause severe pain, characterized by a dull, constant ache with periodic spikes of incident pain.

Spiradenomas (SA) are rare, benign cutaneous adnexal tumors that may progress to become their malignant counterparts, i.e. spiradenocarcinomas (SAC). Cutaneous adnexal tumors are a group of skin tumors consisting of tissues that have differentiated towards one of the four primary adnexal structures found in normal skin: hair follicles, sebaceous sweat glands, apocrine sweat glands, and eccrine sweat glands. SA and SAC tumors were regarded as eccrine gland tumors and termed eccrine spiradenomas and eccrine spiradenocarcinomas, respectively. However, more recent studies have found them to be hair follicle tumors and commonly term them spiradenomas and spiradenocarcinomas, respectively. Further confusing the situation, SA-like and SAC-like tumors are also 1) manifestations of the inherited disorder, CYLD cutaneous syndrome (CCS), and 2) have repeatedly been confused with an entirely different tumor, adenoid cystic carcinomas of the salivary gland. Here, SA and SAC are strictly defined as sporadic hair follicle tumors that do not include the hereditary CCS spiradenomas and heridtary spiradenocarcinoms of CCS or the adenoid cystic carcinomas.

Eccrine carcinoma is a rare skin condition characterized by a plaque or nodule on the scalp, trunk, or extremities. It originates from the eccrine sweat glands of the skin, accounting for less than 0.01% of diagnosed cutaneous malignancies. Eccrine carcinoma tumors are locally aggressive, with a high rate of recurrence. Lack of reliable immunohistochemical markers and similarity to other common tumors has made identification of eccrine carcinoma difficult.

A brain metastasis is a cancer that has metastasized (spread) to the brain from another location in the body and is therefore considered a secondary brain tumor. The metastasis typically shares a cancer cell type with the original site of the cancer. Metastasis is the most common cause of brain cancer, as primary tumors that originate in the brain are less common. The most common sites of primary cancer which metastasize to the brain are lung, breast, colon, kidney, and skin cancer. Brain metastases can occur months or even years after the original or primary cancer is treated. Brain metastases have a poor prognosis for cure, but modern treatments allow patients to live months and sometimes years after the diagnosis.
Large cell lung carcinoma with rhabdoid phenotype (LCLC-RP) is a rare histological form of lung cancer, currently classified as a variant of large cell lung carcinoma (LCLC). In order for a LCLC to be subclassified as the rhabdoid phenotype variant, at least 10% of the malignant tumor cells must contain distinctive structures composed of tangled intermediate filaments that displace the cell nucleus outward toward the cell membrane. The whorled eosinophilic inclusions in LCLC-RP cells give it a microscopic resemblance to malignant cells found in rhabdomyosarcoma (RMS), a rare neoplasm arising from transformed skeletal muscle. Despite their microscopic similarities, LCLC-RP is not associated with rhabdomyosarcoma.
Mucinous cystadenocarcinoma of the lung (MCACL) is a very rare malignant mucus-producing neoplasm arising from the uncontrolled growth of transformed epithelial cells originating in lung tissue.

Adenocarcinoma of the lung is the most common type of lung cancer, and like other forms of lung cancer, it is characterized by distinct cellular and molecular features. It is classified as one of several non-small cell lung cancers (NSCLC), to distinguish it from small cell lung cancer which has a different behavior and prognosis. Lung adenocarcinoma is further classified into several subtypes and variants. The signs and symptoms of this specific type of lung cancer are similar to other forms of lung cancer, and patients most commonly complain of persistent cough and shortness of breath.

Giant-cell carcinoma of the lung (GCCL) is a rare histological form of large-cell lung carcinoma, a subtype of undifferentiated lung cancer, traditionally classified within the non-small-cell lung carcinomas (NSCLC).
Ground-glass opacity (GGO) is a finding seen on chest x-ray (radiograph) or computed tomography (CT) imaging of the lungs. It is typically defined as an area of hazy opacification (x-ray) or increased attenuation (CT) due to air displacement by fluid, airway collapse, fibrosis, or a neoplastic process. When a substance other than air fills an area of the lung it increases that area's density. On both x-ray and CT, this appears more grey or hazy as opposed to the normally dark-appearing lungs. Although it can sometimes be seen in normal lungs, common pathologic causes include infections, interstitial lung disease, and pulmonary edema.
In CT scan of the thyroid, focal and diffuse thyroid abnormalities are commonly encountered. These findings can often lead to a diagnostic dilemma, as the CT reflects nonspecific appearances. Ultrasound (US) examination has a superior spatial resolution and is considered the modality of choice for thyroid evaluation. Nevertheless, CT detects incidental thyroid nodules (ITNs) and plays an important role in the evaluation of thyroid cancer.

A lung cavity or pulmonary cavity is an abnormal, thick-walled, air-filled space within the lung. Cavities in the lung can be caused by infections, cancer, autoimmune conditions, trauma, congenital defects, or pulmonary embolism. The most common cause of a single lung cavity is lung cancer. Bacterial, mycobacterial, and fungal infections are common causes of lung cavities. Globally, tuberculosis is likely the most common infectious cause of lung cavities. Less commonly, parasitic infections can cause cavities. Viral infections almost never cause cavities. The terms cavity and cyst are frequently used interchangeably; however, a cavity is thick walled, while a cyst is thin walled. The distinction is important because cystic lesions are unlikely to be cancer, while cavitary lesions are often caused by cancer.
References
- ↑ Yang, Rong-Hsin; Ting, Chien-Hsin; Chu, Yum-Kung (August 2016). "Cannonball lung metastases as a presenting feature of ectopic hCG expression". Journal of Oncological Sciences. 2 (2–3): 58–62. doi:10.1016/j.jons.2016.07.003.
- 1 2 Ammannagari, Nischala; Polu, Vengamamba (8 January 2013). "'Cannon ball' pulmonary metastases". Case Reports. 2013: bcr2012008158. doi:10.1136/bcr-2012-008158. PMC 3604387 . PMID 23302554.
- ↑ Yudin, Andrey (2014). "Snowstorm Sign and Cannonball Metastases". Metaphorical Signs in Computed Tomography of Chest and Abdomen. p. 27. doi:10.1007/978-3-319-04013-4_14. ISBN 978-3-319-04012-7.
- ↑ Young, Paul (12 October 2018). "Cannon Balls". Life in the Fast Lane • LITFL. Retrieved 17 December 2024.[ self-published source? ]
- ↑ Hla Aye, M T; Rubel, A R; Han, M B; Kyaw, A Y; Mani, B I; Chong, V H (December 2022). "Pulmonary cannonball metastasis and renal cell carcinoma". QJM: An International Journal of Medicine. 115 (12): 856–857. doi:10.1093/qjmed/hcac203. PMID 35993896.
- ↑ Scaramozzino, Marco Umberto; Nassisi, Veronica; Sapone, Giovanni (22 April 2024). "Pulmonary 'cannonball' metastasis from endometrial cancer: a rare case report". Chest Disease Reports. 12. doi:10.4081/cdr.12.12460.