
Plastic surgery is a surgical specialty involving the restoration, reconstruction, or alteration of the human body. It can be divided into two main categories: reconstructive surgery and cosmetic surgery. Reconstructive surgery covers a wide range of specialties, including craniofacial surgery, hand surgery, microsurgery, and the treatment of burns. This category of surgery focuses on restoring a body part or improving its function. In contrast, cosmetic surgery focuses solely on improving the physical appearance of the body. A comprehensive definition of plastic surgery has never been established, because it has no distinct anatomical object and thus overlaps with practically all other surgical specialties. An essential feature of plastic surgery is that it involves the treatment of conditions that require or may require tissue relocation skills.

Rhinoplasty, commonly called nose job, medically called nasal reconstruction, is a plastic surgery procedure for altering and reconstructing the nose. There are two types of plastic surgery used – reconstructive surgery that restores the form and functions of the nose and cosmetic surgery that changes the appearance of the nose. Reconstructive surgery seeks to resolve nasal injuries caused by various traumas including blunt, and penetrating trauma and trauma caused by blast injury. Reconstructive surgery can also treat birth defects, breathing problems, and failed primary rhinoplasties. Rhinoplasty may remove a bump, narrow nostril width, change the angle between the nose and the mouth, or address injuries, birth defects, or other problems that affect breathing, such as a deviated nasal septum or a sinus condition. Surgery only on the septum is called a septoplasty.
Phalloplasty is the construction or reconstruction of a penis or the artificial modification of the penis by surgery. The term is also occasionally used to refer to penis enlargement.
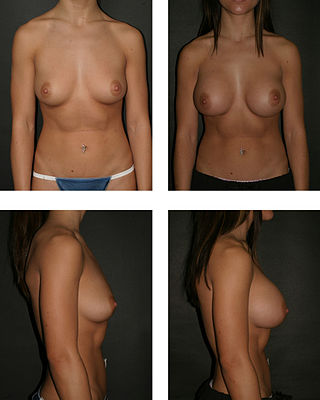
Breast augmentation and augmentation mammoplasty is a cosmetic surgery procedure, which uses breast-implants and/ or fat-graft mammoplasty technique to increase the size, change the shape, and alter the texture of the breasts. Although in some cases augmentation mammoplasty is applied to correct congenital defects of the breasts and the chest wall in other cases it is performed purely for cosmetic reasons.
Otoplasty is a procedure for correcting the deformities and defects of the auricle, whether these defects are congenital conditions or caused by trauma. Otoplastic surgeons may reshape, move, or augment the cartilaginous support framework of the auricle to correct these defects.

A facelift, technically known as a rhytidectomy, is a type of cosmetic surgery procedure intended to give a more youthful facial appearance. There are multiple surgical techniques and exercise routines. Surgery usually involves the removal of excess facial skin, with or without the tightening of underlying tissues, and the redraping of the skin on the patient's face and neck. Exercise routines tone underlying facial muscles without surgery. Surgical facelifts are effectively combined with eyelid surgery (blepharoplasty) and other facial procedures and are typically performed under general anesthesia or deep twilight sleep.
Chondrolaryngoplasty is a surgical procedure in which the thyroid cartilage is reduced in size by shaving down the cartilage through an incision in the throat, generally to aid those who are uncomfortable with the girth of their Adam's apple.

Microtia is a congenital deformity where the auricle is underdeveloped. A completely undeveloped auricle is referred to as anotia. Because microtia and anotia have the same origin, it can be referred to as microtia-anotia. Microtia can be unilateral or bilateral. Microtia occurs in 1 out of about 8,000–10,000 births. In unilateral microtia, the right ear is most commonly affected. It may occur as a complication of taking Accutane (isotretinoin) during pregnancy.

A breast implant is a prosthesis used to change the size, shape, and contour of a person's breast. In reconstructive plastic surgery, breast implants can be placed to restore a natural looking breast following a mastectomy, to correct congenital defects and deformities of the chest wall or, cosmetically, to enlarge the appearance of the breast through breast augmentation surgery.
Mastopexy is the plastic surgery mammoplasty procedure for raising sagging breasts upon the chest of the woman, by changing and modifying the size, contour, and elevation of the breasts. In a breast-lift surgery to re-establish an aesthetically proportionate bust for the woman, the critical corrective consideration is the tissue viability of the nipple-areola complex (NAC), to ensure the functional sensitivity of the breasts for lactation and breast-feeding.

Macrotia refers to an ear that is larger than would be expected. The normal auricular axis length is 58–62 mm (2.3–2.4 in) among females and 62–66 mm (2.4–2.6 in) among males. The average width of an adult ear, specifically the distance between the helix root and the posterior auricle, is between 30 and 40 mm.

Tuberous breasts are a result of a congenital abnormality of the breasts which can occur in both men and women, one breast or both. During puberty breast development is stymied and the breasts fail to develop normally and fully. The exact cause of this is as yet unclear; however, a study in 2011 of the cells in the breasts of both males and females with tubular breasts suggested a genetic link in a disorder of collagen deposition. The condition is thought to affect one to five per cent of breast augmentation patients; however, the proportion of the general population affected is unknown as surgery is not always sought.
Burt Brent is a retired reconstructive plastic surgeon best known for his work in reconstructing the absent outer ear. He built upon the techniques of his mentor, Dr. Radford Tanzer of the Mary Hitchcock Clinic at Dartmouth Medical School and repaired ear defects in 1,800 patients, most of them children born with ear deformities such as microtia. He also reconstructed ears lost or due to some form of trauma.

Cryptotia is the condition where an ear appears to have its upper portion buried underneath the side of the head. The condition also involves underdeveloped scapha and antihelical crura. Cryptotia is also known as buried ear or hidden ear.

Protruding ear, otapostasis or bat ear is an abnormally prominent human ear. It may be unilateral or bilateral. The concha is large with poorly developed antihelix and scapha. It is the result of malformation of cartilage during primitive ear development in intrauterine life. The deformity can be corrected anytime after five years of age. The surgery is preferably done at the earliest possible age in order to avoid psychological distress. Correction by otoplasty involves changing the shape of the ear cartilage so that the ear is brought closer to the side of the head. The skin is not removed, but the shape of the cartilage is altered. The surgery does not affect hearing. It is done for cosmetic purposes only. The complications of the surgery, though rare, are keloid formation, hematoma formation, infection and asymmetry between the ears.
The Merck stitch method is a minimally invasive procedure for pinning protruding ears, developed by W. H. Merck. The method belongs to the special types of ear pinning surgeries. In contrast to other variations of minimally invasive procedures the stitch method does not use additional techniques from the traditional ear pinning surgeries (otoplasty). It belongs to the closed ear pinning surgeries because the ear is not cut open for the placement of the sutures. According to the experience of the author the Stitch Method is suitable for all protruding ears. The stitch method is the most frequently performed otoplasty among the minimally invasive methods.
The Mustardé technique is an otoplastic surgery (otoplasty) for pinning protruding ears. The method belongs together with the Stenström and Converse methods to the traditional otoplasties. It is antihelix plastic surgery performed with the suturing technique.
The Stenström technique or method is otoplastic surgery (otoplasty) for pinning protruding ears. The method belongs together with the Mustardé technique and the Converse technique to the traditional or conventional otoplasties.
The Converse technique, together with the Mustardé technique and Stenström technique, belongs to the standard methods of traditional otoplasty. Numerous variations for pinning ears have been derived from them.
The incisionless Fritsch otoplasty is a minimally invasive procedure for pinning protruding ears.