Related Research Articles
The Duesberg hypothesis is the claim that AIDS is not caused by HIV, but instead that AIDS is caused by noninfectious factors such as recreational and pharmaceutical drug use and that HIV is merely a harmless passenger virus. The hypothesis was popularized by Peter Duesberg, a professor of biology at University of California, Berkeley, from whom the hypothesis gets its name. The scientific consensus is that the Duesberg hypothesis is incorrect and that HIV is the cause of AIDS. The most prominent supporters of the hypothesis are Duesberg himself, biochemist and vitamin proponent David Rasnick, and journalist Celia Farber. The scientific community generally contends that Duesberg's arguments in favor of the hypothesis are the result of cherry-picking predominantly outdated scientific data and selectively ignoring evidence that demonstrates HIV's role in causing AIDS.

HIV/AIDS denialism is the belief, despite conclusive evidence to the contrary, that the human immunodeficiency virus (HIV) does not cause acquired immune deficiency syndrome (AIDS). Some of its proponents reject the existence of HIV, while others accept that HIV exists but argue that it is a harmless passenger virus and not the cause of AIDS. Insofar as they acknowledge AIDS as a real disease, they attribute it to some combination of sexual behavior, recreational drugs, malnutrition, poor sanitation, haemophilia, or the effects of the medications used to treat HIV infection (antiretrovirals).
The spread of HIV/AIDS has affected millions of people worldwide; AIDS is considered a pandemic. The World Health Organization (WHO) estimated that in 2016 there were 36.7 million people worldwide living with HIV/AIDS, with 1.8 million new HIV infections per year and 1 million deaths due to AIDS. Misconceptions about HIV and AIDS arise from several different sources, from simple ignorance and misunderstandings about scientific knowledge regarding HIV infections and the cause of AIDS to misinformation propagated by individuals and groups with ideological stances that deny a causative relationship between HIV infection and the development of AIDS. Below is a list and explanations of some common misconceptions and their rebuttals.

Simian immunodeficiency virus (SIV) is a species of retrovirus that cause persistent infections in at least 45 species of non-human primates. Based on analysis of strains found in four species of monkeys from Bioko Island, which was isolated from the mainland by rising sea levels about 11,000 years ago, it has been concluded that SIV has been present in monkeys and apes for at least 32,000 years, and probably much longer.

Sir Peter Karel, Baron Piot, is a Belgian-British microbiologist known for his research into Ebola and AIDS.
AIDS is caused by a human immunodeficiency virus (HIV), which originated in non-human primates in Central and West Africa. While various sub-groups of the virus acquired human infectivity at different times, the present pandemic had its origins in the emergence of one specific strain – HIV-1 subgroup M – in Léopoldville in the Belgian Congo in the 1920s.

The global pandemic of HIV/AIDS began in 1981, and is an ongoing worldwide public health issue. According to the World Health Organization (WHO), by 2023, HIV/AIDS had killed approximately 40.4 million people, and approximately 39 million people were infected with HIV globally. Of these, 29.8 million people (75%) are receiving antiretroviral treatment. There were about 630,000 deaths from HIV/AIDS in 2022. The 2015 Global Burden of Disease Study estimated that the global incidence of HIV infection peaked in 1997 at 3.3 million per year. Global incidence fell rapidly from 1997 to 2005, to about 2.6 million per year. Incidence of HIV has continued to fall, decreasing by 23% from 2010 to 2020, with progress dominated by decreases in Eastern Africa and Southern Africa. As of 2020, there are approximately 1.5 million new infections of HIV per year globally.
Following infection with HIV-1, the rate of clinical disease progression varies between individuals. Factors such as host susceptibility, genetics and immune function, health care and co-infections as well as viral genetic variability may affect the rate of progression to the point of needing to take medication in order not to develop AIDS.

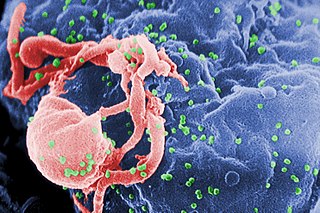
The human immunodeficiency virus (HIV) is a retrovirus that attacks the immune system. It can be managed with treatment. Without treatment it can lead to a spectrum of conditions including acquired immunodeficiency syndrome (AIDS).
HIV/AIDS was recognised as a novel illness in the early 1980s. An AIDS case is classified as "early" if the death occurred before 5 June 1981, when the AIDS epidemic was formally recognized by medical professionals in the United States.

The subtypes of HIV include two main subtypes, known as HIV type 1 (HIV-1) and HIV type 2 (HIV-2). These subtypes have distinct genetic differences and are associated with different epidemiological patterns and clinical characteristics.
Kinshasa General Hospital is a hospital located in the Gombe commune of Kinshasa, Democratic Republic of Congo. Before the ousting of President Mobutu Sese Seko, it was known as Mama Yemo Hospital after the president's mother. The 2000-bed hospital registers over 3,000 consultations daily. It was one of the first places where AIDS was observed.

The Democratic Republic of the Congo was one of the first African countries to recognize HIV, registering cases of HIV among hospital patients as early as 1983.
Although Senegal is a relatively underdeveloped country, HIV prevalence in the general population is low at around 0.08 per 1000 people, under 1% of the population. This relatively low prevalence rate is aided by the fact that few people are infected every year – in 2016, 1100 new cases were reported vs 48,000 new cases in Brazil. Senegal's death due to HIV rate, particularly when compared it to its HIV prevalence rate, is relatively high with 1600 deaths in 2016. Almost two times as many women were infected with HIV as men in 2016, and while almost three times as many women were receiving antiretroviral therapy (ARV) as men, only 52% of HIV positive people in Senegal received ARV treatment in 2016.
Project SIDA (1984–1991), or Projet SIDA, was a joint scientific project between Zaire, the United States, and Belgium to study AIDS in Central Africa. Headquartered in Kinshasa, Zaire (DRC), Projet SIDA was designed as a collaboration between foreign scientists with experience studying epidemics and local scientists and physicians familiar with the local culture and customs. Initiated in 1984, Project SIDA began under the direction of Jonathan Mann with funding from the U.S. and Belgium, as well as support from the Zairian government. Project SIDA was based at Mama Yemo hospital in Kinshasa.
Fred Mhalu is a microbiologist and medical researcher from Tanzania. His main area of study revolves around infectious diseases and intervention. Ever since 1986, he has been a main contributor to the information about AIDS in Africa. As a co-coordinator of a Tanzanian-Swedish research collaboration called TANSWED, he was involved in many research projects that lead to multiple publications in medical journals. His more recent research on HIV/AIDS involves studying breast cancer in HIV prevalent areas, evaluating prevention of mother-to-child-transmission of HIV-1, and observing sexual behaviors of high risk populations for HIV-1.
Bila M. Kapita is a doctor from Kinshasa, Democratic Republic of the Congo who aided in initial research efforts investigating HIV/AIDS in Africa in the 1980s and 1990s. Kapita is credited as one of the first African scientists to independently identify that AIDS was prevalent in Central Africa. Research work in collaboration with Project SIDA helped identify and publicize the heterosexual sexual transmission of HIV. Following his research career, he continued caring for patients with HIV/AIDS and has more recently returned to practicing cardiology.

Souleymane Mboup is a Senegalese microbiologist, medical researcher, and colonel in the Armed Forces of Senegal. In 1985, he was a member of the first team to identify HIV-2, a form of HIV that is typically found in West Africa and is less transmissible than the more common HIV-1. Mboup has contributed to the improvement of Senegal's research infrastructure throughout his career. Among his published works, he is known for editing the 1994 reference book AIDS in Africa. Mboup is currently the President of L'Institut de Recherche en Santé, de Surveillance Épidémiologique et de Formations (IRESSEF) in Diamniadio, Senegal.

In August–November 1976, an outbreak of Ebola virus disease occurred in Zaire. The first recorded case was from Yambuku, a small village in Mongala District, 1,098 kilometres (682 mi) northeast of the capital city of Kinshasa.

Godefridus Johannes Petrus "Frits" van Griensven is a pioneering Dutch scientist in epidemiology, sociology and public health. Most of his work is on addressing the HIV epidemic among men who have sex with men and other HIV key populations.
References
- ↑ "Nzila Nzilambi's research works | University of Kinshasa, Kinshasa (UNIKIN) and other places". ResearchGate. Retrieved 2020-06-15.
- ↑ Colebunders, Robert; Francis, Henry; Izaley, Lebughe; Kabasele, Kanyinda; Nzilambi, Nzila; Van Der Groen, Guido; Vercauteren, Gaby; Mann, JonathanM.; Bila, Kapita; Kakonde, Ndangi; Ifoto, Limbaka (February 1987). "Evaluation of a Clinical Case-Definition of Acquired Immunodeficiency Syndrome in Africa". The Lancet. 329 (8531): 492–494. doi:10.1016/s0140-6736(87)92099-x. ISSN 0140-6736. PMID 2881049. S2CID 659937.
- ↑ Noble, Kenneth B. (1994-03-22). "Political Chaos in Zaire Disrupts Efforts to Control AIDS Epidemic". The New York Times. ISSN 0362-4331 . Retrieved 2020-09-28.
- ↑ Ap (1988-02-04). "Study Backs Theory That AIDS Festered in Africa". The New York Times. ISSN 0362-4331 . Retrieved 2020-06-24.
- ↑ Gerhart, Gail M.; Richburg, Keith B. (1997). "Out of America: A Black Man Confronts Africa". Foreign Affairs. 76 (6): 176. doi:10.2307/20048340. ISSN 0015-7120. JSTOR 20048340.
- ↑ Garrett, Laurie (1994). The Coming Plague: Newly Emerging Diseases in a World Out of Balance. Macmillan. ISBN 978-0-374-12646-9.
- ↑ Cohen, Jon (1997). "The Rise and Fall of Projet SIDA". Science. 278 (5343): 1565–1568. doi:10.1126/science.278.5343.1565. ISSN 0036-8075. JSTOR 2894851. PMID 9411779. S2CID 26805248.
- ↑ Mann, J. M. (1986-06-20). "Surveillance for AIDS in a central African city. Kinshasa, Zaire". JAMA: The Journal of the American Medical Association. 255 (23): 3255–3259. doi:10.1001/jama.255.23.3255. PMID 3012131.
- ↑ Nzilambi, Nzila; De Cock, Kevin M.; Forthal, Donald N.; Francis, Henry; Ryder, Robert W.; Malebe, Ismey; Getchell, Jane; Laga, Marie; Piot, Peter; McCormick, Joseph B. (1988-02-04). "The Prevalence of Infection with Human Immunodeficiency Virus over a 10-Year Period in Rural Zaire". New England Journal of Medicine. 318 (5): 276–279. doi:10.1056/NEJM198802043180503. ISSN 0028-4793. PMID 3336420.
- ↑ Mann, J. M. (1986-06-20). "Surveillance for AIDS in a central African city. Kinshasa, Zaire". JAMA: The Journal of the American Medical Association. 255 (23): 3255–3259. doi:10.1001/jama.255.23.3255. PMID 3012131.
This article needs additional or more specific categories .(November 2022) |