Related Research Articles

In human anatomy, the arm refers to the upper limb in common usage, although academically the term specifically means the upper arm between the glenohumeral joint and the elbow joint. The distal part of the upper limb between the elbow and the radiocarpal joint is known as the forearm or "lower" arm, and the extremity beyond the wrist is the hand.

The radial nerve is a nerve in the human body that supplies the posterior portion of the upper limb. It innervates the medial and lateral heads of the triceps brachii muscle of the arm, as well as all 12 muscles in the posterior osteofascial compartment of the forearm and the associated joints and overlying skin.

The median nerve is a nerve in humans and other animals in the upper limb. It is one of the five main nerves originating from the brachial plexus.

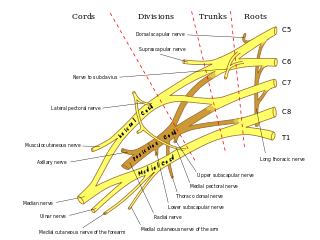
The brachial plexus is a network of nerves formed by the anterior rami of the lower four cervical nerves and first thoracic nerve. This plexus extends from the spinal cord, through the cervicoaxillary canal in the neck, over the first rib, and into the armpit, it supplies afferent and efferent nerve fibers to the chest, shoulder, arm, forearm, and hand.

The phrenic nerve is a mixed motor/sensory nerve that originates from the C3-C5 spinal nerves in the neck. The nerve is important for breathing because it provides exclusive motor control of the diaphragm, the primary muscle of respiration. In humans, the right and left phrenic nerves are primarily supplied by the C4 spinal nerve, but there is also a contribution from the C3 and C5 spinal nerves. From its origin in the neck, the nerve travels downward into the chest to pass between the heart and lungs towards the diaphragm.
The long thoracic nerve is a branch of the brachial plexus derived from cervical nerves C5-C7 that innervates the serratus anterior muscle.
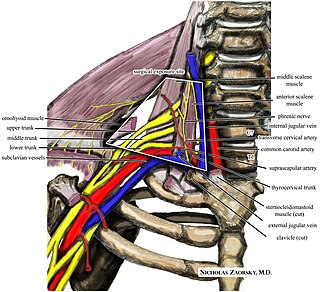
Thoracic outlet syndrome (TOS) is a condition in which there is compression of the nerves, arteries, or veins in the superior thoracic aperture, the passageway from the lower neck to the armpit, also known as the thoracic outlet. There are three main types: neurogenic, venous, and arterial. The neurogenic type is the most common and presents with pain, weakness, paraesthesia, and occasionally loss of muscle at the base of the thumb. The venous type results in swelling, pain, and possibly a bluish coloration of the arm. The arterial type results in pain, coldness, and pallor of the arm.
Axonotmesis is an injury to the peripheral nerve of one of the extremities of the body. The axons and their myelin sheath are damaged in this kind of injury, but the endoneurium, perineurium and epineurium remain intact. Motor and sensory functions distal to the point of injury are completely lost over time leading to Wallerian degeneration due to ischemia, or loss of blood supply. Axonotmesis is usually the result of a more severe crush or contusion than neurapraxia.
The musculocutaneous nerve is a mixed branch of the lateral cord of the brachial plexus derived from cervical spinal nerves C5-C7. It arises opposite the lower border of the pectoralis major. It provides motor innervation to the muscles of the anterior compartment of the arm: the coracobrachialis, biceps brachii, and brachialis. It provides sensory innervation to the lateral forearm. It courses through the anterior part of the arm, terminating 2 cm above elbow; after passing the lateral edge of the tendon of biceps brachii it is becomes known as the lateral cutaneous nerve of the forearm.
Klumpke's paralysis is a variety of partial palsy of the lower roots of the brachial plexus. The brachial plexus is a network of spinal nerves that originates in the back of the neck, extends through the axilla (armpit), and gives rise to nerves to the upper limb. The paralytic condition is named after Augusta Déjerine-Klumpke.
Erb's palsy is a paralysis of the arm caused by injury to the upper group of the arm's main nerves, specifically the severing of the upper trunk C5–C6 nerves. These form part of the brachial plexus, comprising the ventral rami of spinal nerves C5–C8 and thoracic nerve T1. These injuries arise most commonly, but not exclusively, from shoulder dystocia during a difficult birth. Depending on the nature of the damage, the paralysis can either resolve on its own over a period of months, necessitate rehabilitative therapy, or require surgery.
In medicine, a stinger, also called a burner or nerve pinch injury, is a neurological injury suffered by athletes, mostly in high-contact sports such as ice hockey, rugby, American football, and wrestling. The spine injury is characterized by a shooting or stinging pain that travels down one arm, followed by numbness and weakness in the parts of the arms, including the biceps, deltoid, and spinati muscles. Many athletes in contact sports have suffered stingers, but they are often unreported to medical professionals.

Monoplegia is paralysis of a single limb, usually an arm. Common symptoms associated with monoplegic patients are weakness, numbness, and pain in the affected limb. Monoplegia is a type of paralysis that falls under hemiplegia. While hemiplegia is paralysis of half of the body, monoplegia is localized to a single limb or to a specific region of the body. Monoplegia of the upper limb is sometimes referred to as brachial monoplegia, and that of the lower limb is called crural monoplegia. Monoplegia in the lower extremities is not as common of an occurrence as in the upper extremities. Monoparesis is a similar, but less severe, condition because one limb is very weak, not paralyzed. For more information, see paresis.
A brachial plexus injury (BPI), also known as brachial plexus lesion, is an injury to the brachial plexus, the network of nerves that conducts signals from the spinal cord to the shoulder, arm and hand. These nerves originate in the fifth, sixth, seventh and eighth cervical (C5–C8), and first thoracic (T1) spinal nerves, and innervate the muscles and skin of the chest, shoulder, arm and hand.

Progressive muscular atrophy (PMA), also called Duchenne–Aran disease and Duchenne–Aran muscular atrophy, is a disorder characterised by the degeneration of lower motor neurons, resulting in generalised, progressive loss of muscle function.
Parsonage–Turner syndrome, also known as acute brachial neuropathy, neuralgic amyotrophy and abbreviated PTS, is a syndrome of unknown cause; although many specific risk factors have been identified, the cause is still unknown. The condition manifests as a set of symptoms most likely resulting from autoimmune inflammation of unknown cause of the brachial plexus.

Amyotrophic lateral sclerosis (ALS), also known as motor neurone disease (MND) or Lou Gehrig's disease in the United States, is a rare, terminal neurodegenerative disorder that results in the progressive loss of both upper and lower motor neurons that normally control voluntary muscle contraction. ALS is the most common form of the motor neuron diseases. ALS often presents in its early stages with gradual muscle stiffness, twitches, weakness, and wasting. Motor neuron loss typically continues until the abilities to eat, speak, move, and, lastly, breathe are all lost. While only 15% of people with ALS also fully develop frontotemporal dementia, an estimated 50% face at least some minor difficulties with thinking and behavior. Depending on which of the aforementioned symptoms develops first, ALS is classified as limb-onset or bulbar-onset.

Brachial plexus block is a regional anesthesia technique that is sometimes employed as an alternative or as an adjunct to general anesthesia for surgery of the upper extremity. This technique involves the injection of local anesthetic agents in close proximity to the brachial plexus, temporarily blocking the sensation and ability to move the upper extremity. The subject can remain awake during the ensuing surgical procedure, or they can be sedated or even fully anesthetized if necessary.

Radiation-induced lumbar plexopathy (RILP) or radiation-induced lumbosacral plexopathy (RILSP) is nerve damage in the pelvis and lower spine area caused by therapeutic radiation treatments. RILP is a rare side effect of external beam radiation therapy and both interstitial and intracavity brachytherapy radiation implants.
Brachial amyotrophic diplegia, also called Vulpian-Bernhardt Syndrome (VBS), flail arm syndrome, or man-in-barrel syndrome, is a rare motor neuron disease, often considered to be a phenotype or regional variant of amyotrophic lateral sclerose. In the first twelve to eighteen months, only a progressive weakness of one or both arms is observed. Within the spectrum of ALS, this subtype has a relatively longer survival time. Because of its distinct symptoms, it was suggested that VBS is a separate entity, different from ALS.
References
- 1 2 Yeoman, P. M.; Seddon, H. J. (August 1961). "Brachial Plexus Injuries: Treatment of the Flail Arm". The Journal of Bone and Joint Surgery. British Volume. 43-B (3): 493–500. doi:10.1302/0301-620X.43B3.493.
- ↑ Althausen, Peter L.; Lee, Mark A.; Finkemeier, Christopher G. (November 2003). "Scapulothoracic Dissociation: Diagnosis and Treatment". Clinical Orthopaedics and Related Research. 416 (416): 237–244. doi:10.1097/01.blo.0000093022.56370.fe. PMID 14646766. S2CID 24993921.
- ↑ Wilkinson, M. C. P.; Birch, R.; Bonney, G. (1 October 1993). "Brachial plexus injury: when to amputate?". Injury. 24 (9): 603–605. doi:10.1016/0020-1383(93)90123-N. PMID 8288380.
| | This article about a medical condition affecting the nervous system is a stub. You can help Wikipedia by expanding it. |