Related Research Articles
Cranial nerves are the nerves that emerge directly from the brain, of which there are conventionally considered twelve pairs. Cranial nerves relay information between the brain and parts of the body, primarily to and from regions of the head and neck, including the special senses of vision, taste, smell, and hearing.

The pupil is a black hole located in the center of the iris of the eye that allows light to strike the retina. It appears black because light rays entering the pupil are either absorbed by the tissues inside the eye directly, or absorbed after diffuse reflections within the eye that mostly miss exiting the narrow pupil. The term "pupil" was coined by Gerard of Cremona.
Mydriasis is the dilation of the pupil, usually having a non-physiological cause, or sometimes a physiological pupillary response. Non-physiological causes of mydriasis include disease, trauma, or the use of drugs.

The oculomotor nerve is the third cranial nerve. It enters the orbit through the superior orbital fissure and innervates extrinsic eye muscles that enable most movements of the eye and that raise the eyelid. The nerve also contains fibers that innervate the intrinsic eye muscles that enable pupillary constriction and accommodation. The oculomotor nerve is derived from the basal plate of the embryonic midbrain. Cranial nerves IV and VI also participate in control of eye movement.

The pupillary light reflex (PLR) or photopupillary reflex is a reflex that controls the diameter of the pupil, in response to the intensity (luminance) of light that falls on the retinal ganglion cells of the retina in the back of the eye, thereby assisting in adaptation of vision to various levels of lightness/darkness. A greater intensity of light causes the pupil to constrict, whereas a lower intensity of light causes the pupil to dilate. Thus, the pupillary light reflex regulates the intensity of light entering the eye. Light shone into one eye will cause both pupils to constrict.

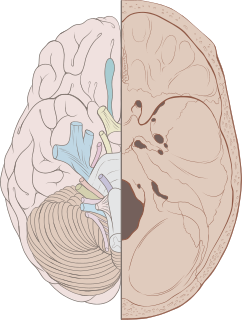
The fibers of the oculomotor nerve arise from a nucleus in the midbrain, which lies in the gray substance of the floor of the cerebral aqueduct and extends in front of the aqueduct for a short distance into the floor of the third ventricle. From this nucleus the fibers pass forward through the tegmentum, the red nucleus, and the medial part of the substantia nigra, forming a series of curves with a lateral convexity, and emerge from the oculomotor sulcus on the medial side of the cerebral peduncle.
Miosis, or myosis, is excessive constriction of the pupil. The term is from Ancient Greek μύειν mūein, "to close the eyes". The opposite condition, mydriasis, is the dilation of the pupil. Anisocoria is the condition of one pupil being more dilated than the other.
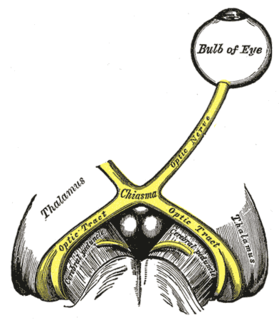
The optic tract is a part of the visual system in the brain. It is a continuation of the optic nerve that relays information from the optic chiasm to the ipsilateral lateral geniculate nucleus (LGN), pretectal nuclei, and superior colliculus.

Horner's syndrome, also known as oculosympathetic paresis, is a combination of symptoms that arises when a group of nerves known as the sympathetic trunk is damaged. The signs and symptoms occur on the same side (ipsilateral) as it is a lesion of the sympathetic trunk. It is characterized by miosis, partial ptosis, apparent anhydrosis, with apparent enophthalmos.
The Edinger–Westphal nucleus is the parasympathetic pre-ganglionic nucleus that innervates the iris sphincter muscle and the ciliary muscle.

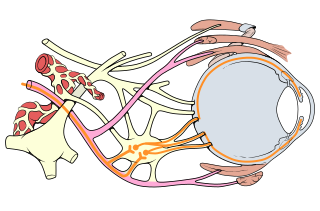
The ciliary ganglion is a bundle of nerve parasympathetic ganglion located just behind the eye in the posterior orbit. It is 1–2 mm in diameter and in humans contains approximately 2,500 neurons. The ganglion contains postganglionic parasympathetic neurons. These neurons supply the pupillary sphincter muscle, which constricts the pupil, and the ciliary muscle which contracts to make the lens more convex. Both of these muscles are involuntary since they are controlled by the parasympathetic division of the autonomic nervous system.

The iris sphincter muscle is a muscle in the part of the eye called the iris. It encircles the pupil of the iris, appropriate to its function as a constrictor of the pupil.

Adie syndrome, also known as Holmes-Adie syndrome, is a neurological disorder characterized by a tonically dilated pupil that reacts slowly to light but shows a more definite response to accommodation. It is frequently seen in females with absent knee or ankle jerks and impaired sweating.

Brain herniation is a potentially deadly side effect of very high pressure within the skull that occurs when a part of the brain is squeezed across structures within the skull. The brain can shift across such structures as the falx cerebri, the tentorium cerebelli, and even through the foramen magnum. Herniation can be caused by a number of factors that cause a mass effect and increase intracranial pressure (ICP): these include traumatic brain injury, intracranial hemorrhage, or brain tumor.

Anisocoria is a condition characterized by an unequal size of the eyes' pupils. Affecting up to 20% of the population, anisocoria is often entirely harmless, but can be a sign of more serious medical problems.

The branches of the ciliary ganglion are the short ciliary nerves.
A relative afferent pupillary defect (RAPD), also known as a Marcus Gunn pupil, is a medical sign observed during the swinging-flashlight test whereupon the patient's pupils dilate when a bright light is swung from the unaffected eye to the affected eye. The affected eye still senses the light and produces pupillary sphincter constriction to some degree, albeit reduced.
Oculomotor nerve palsy is an eye condition resulting from damage to the third cranial nerve or a branch thereof. As the name suggests, the oculomotor nerve supplies the majority of the muscles controlling eye movements. Thus, damage to this nerve will result in the affected individual being unable to move their eye normally. In addition, the nerve also supplies the upper eyelid muscle and It is accompanied by parasympathetic fibers innervating the muscles responsible for pupil constriction. The limitations of eye movements resulting from the condition are generally so severe that the affected individual is unable to maintain normal alignment of their eyes when looking straight ahead, leading to strabismus and, as a consequence, double vision (diplopia).

Pupillary response is a physiological response that varies the size of the pupil, via the optic and oculomotor cranial nerve.

The ciliary ganglion is a parasympathetic ganglion located just behind the eye in the posterior orbit. Three types of axons enter the ciliary ganglion but only the preganglionic parasympathetic axons synapse there. The entering axons are arranged into three roots of the ciliary ganglion, which join enter the posterior surface of the ganglion.
References
- ↑ Dr. Aruj Khurana. "Concussion injuries to the brain". Comprehensive Ophthalmology (fourth ed.). New Age International (P): 311.