Related Research Articles

Hypoxia is a condition in which the body or a region of the body is deprived of adequate oxygen supply at the tissue level. Hypoxia may be classified as either generalized, affecting the whole body, or local, affecting a region of the body. Although hypoxia is often a pathological condition, variations in arterial oxygen concentrations can be part of the normal physiology, for example, during strenuous physical exercise.

Tumor hypoxia is the situation where tumor cells have been deprived of oxygen. As a tumor grows, it rapidly outgrows its blood supply, leaving portions of the tumor with regions where the oxygen concentration is significantly lower than in healthy tissues. Hypoxic microenvironments in solid tumors are a result of available oxygen being consumed within 70 to 150 μm of tumor vasculature by rapidly proliferating tumor cells thus limiting the amount of oxygen available to diffuse further into the tumor tissue. In order to support continuous growth and proliferation in challenging hypoxic environments, cancer cells are found to alter their metabolism. Furthermore, hypoxia is known to change cell behavior and is associated with extracellular matrix remodeling and increased migratory and metastatic behavior.
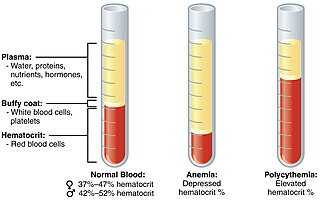
Polycythemia is a laboratory finding in which the hematocrit and/or hemoglobin concentration are increased in the blood. Polycythemia is sometimes called erythrocytosis, and there is significant overlap in the two findings, but the terms are not the same: polycythemia describes any increase in hematocrit and/or hemoglobin, while erythrocytosis describes an increase specifically in the number of red blood cells in the blood.

Generalized hypoxia is a medical condition in which the tissues of the body are deprived of the necessary levels of oxygen due to an insufficient supply of oxygen, which may be due to the composition or pressure of the breathing gas, decreased lung ventilation, or respiratory disease, any of which may cause a lower than normal oxygen content in the arterial blood, and consequently a reduced supply of oxygen to all tissues perfused by the arterial blood. This usage is in contradistinction to localized hypoxia, in which only an associated group of tissues, usually with a common blood supply, are affected, usually due to an insufficient or reduced blood supply to those tissues. Generalized hypoxia is also used as a synonym for hypoxic hypoxia This is not to be confused with hypoxemia, which refers to low levels of oxygen in the blood, although the two conditions often occur simultaneously, since a decrease in blood oxygen typically corresponds to a decrease in oxygen in the surrounding tissue. However, hypoxia may be present without hypoxemia, and vice versa, as in the case of infarction. Several other classes of medical hypoxia exist.

Altitude training is the practice by some endurance athletes of training for several weeks at high altitude, preferably over 2,400 metres (8,000 ft) above sea level, though more commonly at intermediate altitudes due to the shortage of suitable high-altitude locations. At intermediate altitudes, the air still contains approximately 20.9% oxygen, but the barometric pressure and thus the partial pressure of oxygen is reduced.

High-altitude pulmonary edema (HAPE) is a life-threatening form of non-cardiogenic pulmonary edema that occurs in otherwise healthy people at altitudes typically above 2,500 meters (8,200 ft). However, cases have also been reported between 1,500–2,500 metres or 4,900–8,200 feet in more vulnerable subjects.

Cerebral hypoxia is a form of hypoxia, specifically involving the brain; when the brain is completely deprived of oxygen, it is called cerebral anoxia. There are four categories of cerebral hypoxia; they are, in order of increasing severity: diffuse cerebral hypoxia (DCH), focal cerebral ischemia, cerebral infarction, and global cerebral ischemia. Prolonged hypoxia induces neuronal cell death via apoptosis, resulting in a hypoxic brain injury.
Hypoxic pulmonary vasoconstriction (HPV), also known as the Euler-Liljestrand mechanism, is a physiological phenomenon in which small pulmonary arteries constrict in the presence of alveolar hypoxia. By redirecting blood flow from poorly-ventilated lung regions to well-ventilated lung regions, HPV is thought to be the primary mechanism underlying ventilation/perfusion matching.

Hypoxemia is an abnormally low level of oxygen in the blood. More specifically, it is oxygen deficiency in arterial blood. Hypoxemia has many causes, and often causes hypoxia as the blood is not supplying enough oxygen to the tissues of the body.

Intrauterine hypoxia occurs when the fetus is deprived of an adequate supply of oxygen. It may be due to a variety of reasons such as prolapse or occlusion of the umbilical cord, placental infarction, maternal diabetes and maternal smoking. Intrauterine growth restriction may cause or be the result of hypoxia. Intrauterine hypoxia can cause cellular damage that occurs within the central nervous system. This results in an increased mortality rate, including an increased risk of sudden infant death syndrome (SIDS). Oxygen deprivation in the fetus and neonate have been implicated as either a primary or as a contributing risk factor in numerous neurological and neuropsychiatric disorders such as epilepsy, attention deficit hyperactivity disorder, eating disorders and cerebral palsy.
Chronic mountain sickness (CMS) is a disease in which the proportion of blood volume that is occupied by red blood cells increases (polycythaemia) and there is an abnormally low level of oxygen in the blood (hypoxemia). CMS typically develops after extended time living at high altitude. It is most common amongst native populations of high altitude nations. The most frequent symptoms of CMS are headache, dizziness, tinnitus, breathlessness, palpitations, sleep disturbance, fatigue, loss of appetite, confusion, cyanosis, and dilation of veins.

Christian James Lambertsen was an American environmental medicine and diving medicine specialist who was principally responsible for developing the United States Navy frogmen's rebreathers in the early 1940s for underwater warfare. Lambertsen designed a series of rebreathers in 1940 and in 1944 and first called his invention breathing apparatus. Later, after the war, he called it Laru and finally, in 1952, he changed his invention's name again to SCUBA. Although diving regulator technology was invented by Émile Gagnan and Jacques-Yves Cousteau in 1943 and was unrelated to rebreathers, the current use of the word SCUBA is largely attributed to the Gagnan-Cousteau invention. The US Navy considers Lambertsen to be "the father of the Frogmen".

The effects of high altitude on humans are mostly the consequences of reduced partial pressure of oxygen in the atmosphere. The medical problems that are direct consequence of high altitude are caused by the low inspired partial pressure of oxygen, which is caused by the reduced atmospheric pressure, and the constant gas fraction of oxygen in atmospheric air over the range in which humans can survive. The other major effect of altitude is due to lower ambient temperature.
A hypoxicator is a medical device intended to provide a stimulus for the adaptation of an individual's cardiovascular system by means of breathing reduced oxygen hypoxic air and triggering mechanisms of compensation. The aim of intermittent hypoxic training or hypoxic therapy conducted with such a device is to obtain benefits in physical performance and wellbeing through improved oxygen metabolism.
Efaproxiral (INN) is an analogue of the cholesterol drug bezafibrate developed for the treatment of depression, traumatic brain injury, ischemia, stroke, myocardial infarction, diabetes, hypoxia, sickle cell disease, hypercholesterolemia and as a radio sensitiser.
The Hypoxic Training index (HTi) provides an objective measure of the hypoxic stress delivered during the Intermittent Hypoxic Training (IHT) session, compared to simple recording the inhaled fraction of oxygen (FiO2). HTi provides a figure (index) of dosage received by the individual at the end of the session. Knowledge of HTi can therefore be used to alter the training regime for different individuals, compensating for individual variability, and can be used in scientific studies to ensure that subject exposure was correctly controlled.

Organisms can live at high altitude, either on land, in water, or while flying. Decreased oxygen availability and decreased temperature make life at such altitudes challenging, though many species have been successfully adapted via considerable physiological changes. As opposed to short-term acclimatisation, high-altitude adaptation means irreversible, evolved physiological responses to high-altitude environments, associated with heritable behavioural and genetic changes. Among vertebrates, only few mammals and certain birds are known to have completely adapted to high-altitude environments.
Fish are exposed to large oxygen fluctuations in their aquatic environment since the inherent properties of water can result in marked spatial and temporal differences in the concentration of oxygen. Fish respond to hypoxia with varied behavioral, physiological, and cellular responses to maintain homeostasis and organism function in an oxygen-depleted environment. The biggest challenge fish face when exposed to low oxygen conditions is maintaining metabolic energy balance, as 95% of the oxygen consumed by fish is used for ATP production releasing the chemical energy of nutrients through the mitochondrial electron transport chain. Therefore, hypoxia survival requires a coordinated response to secure more oxygen from the depleted environment and counteract the metabolic consequences of decreased ATP production at the mitochondria.
High-altitude adaptation in humans is an instance of evolutionary modification in certain human populations, including those of Tibet in Asia, the Andes of the Americas, and Ethiopia in Africa, who have acquired the ability to survive at altitudes above 2,500 meters. This adaptation means irreversible, long-term physiological responses to high-altitude environments, associated with heritable behavioural and genetic changes. While the rest of the human population would suffer serious health consequences, the indigenous inhabitants of these regions thrive well in the highest parts of the world. These humans have undergone extensive physiological and genetic changes, particularly in the regulatory systems of oxygen respiration and blood circulation, when compared to the general lowland population.
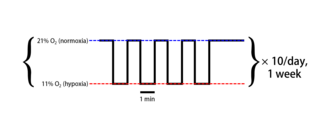
Intermittent hypoxia (also known as episodic hypoxia) is an intervention in which a person or animal undergoes alternating periods of normoxia and hypoxia. Normoxia is defined as exposure to oxygen levels normally found in Earth's atmosphere (~21% O2) and hypoxia as any oxygen levels lower than those of normoxia. Normally, exposure to hypoxia is negatively associated to physiological changes to the body, such as altitude sickness. However, when used in moderation, intermittent hypoxia may be used clinically as a means to alleviate various pathological conditions.
References
- ↑ Navarrete-Opazo, Angela; Mitchell, Gordon S. (15 November 2014). "Therapuetic potential of intermittent hypoxia: a matter of dose". Am J Physiol Regul Integr Comp Physiol. 307 (10): R1181–R1197. doi:10.1152/ajpregu.00208.2014. PMC 4315448 . PMID 25231353.
- ↑ Manukhina EB, Downey HF, Mallet RT (April 2006). "Formation and Role of Nitric Oxide Stores in Adaptation to Hypoxia". Oxygen Transport to Tissue XXVII. Advances in Experimental Medicine and Biology. Vol. 231. pp. 343–65. doi:10.1007/0-387-29540-2_6. ISBN 978-0-387-29543-5. PMID 16565431.
{{cite book}}:|journal=ignored (help) - ↑ Gore CJ, Clark SA, Saunders PU (September 2007). "Nonhematological mechanisms of improved sea-level performance after hypoxic exposure". Medicine and Science in Sports and Exercise. 39 (9): 1600–9. doi: 10.1249/mss.0b013e3180de49d3 . PMID 17805094.
- ↑ Serebrovskaya TV, Manukhina EB, Smith ML, Downey HF, Mallet RT (June 2008). "Intermittent hypoxia: cause of or therapy for systemic hypertension?". Experimental Biology and Medicine. 233 (6): 627–50. doi:10.3181/0710-MR-267. PMID 18408145. S2CID 20045656.
- ↑ Levine, BD (2002). "Intermittent hypoxic training: fact and fancy". High Altitude Medicine & Biology. 3 (2): 177–93. doi:10.1089/15270290260131911. PMID 12162862.
- ↑ Serebrovskaya TV (2002). "Intermittent hypoxia research in the former soviet union and the commonwealth of independent States: history and review of the concept and selected applications". High Altitude Medicine & Biology. 3 (2): 205–21. doi:10.1089/15270290260131939. PMID 12162864. S2CID 28834625.