Related Research Articles

The lungs are the primary organs of the respiratory system in many animals, including humans. In mammals and most other tetrapods, two lungs are located near the backbone on either side of the heart. Their function in the respiratory system is to extract oxygen from the atmosphere and transfer it into the bloodstream, and to release carbon dioxide from the bloodstream into the atmosphere, in a process of gas exchange. Respiration is driven by different muscular systems in different species. Mammals, reptiles and birds use their musculoskeletal systems to support and foster breathing. In early tetrapods, air was driven into the lungs by the pharyngeal muscles via buccal pumping, a mechanism still seen in amphibians. In humans, the primary muscle that drives breathing is the diaphragm. The lungs also provide airflow that makes vocalisation including speech possible.

A bronchus is a passage or airway in the lower respiratory tract that conducts air into the lungs. The first or primary bronchi to branch from the trachea at the carina are the right main bronchus and the left main bronchus. These are the widest bronchi, and enter the right lung, and the left lung at each hilum. The main bronchi branch into narrower secondary bronchi or lobar bronchi, and these branch into narrower tertiary bronchi or segmental bronchi. Further divisions of the segmental bronchi are known as 4th order, 5th order, and 6th order segmental bronchi, or grouped together as subsegmental bronchi. The bronchi, when too narrow to be supported by cartilage, are known as bronchioles. No gas exchange takes place in the bronchi.
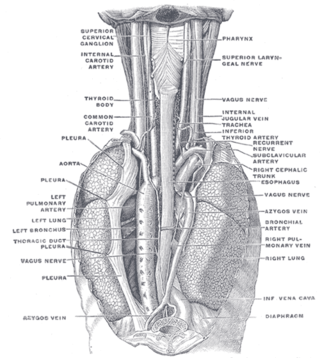
The azygos vein is a vein running up the right side of the thoracic vertebral column draining itself towards the superior vena cava. It connects the systems of superior vena cava and inferior vena cava and can provide an alternative path for blood to the right atrium when either of the venae cavae is blocked.
In medical or research imaging, an incidental imaging finding is an unanticipated finding which is not related to the original diagnostic inquiry. As with other types of incidental medical findings, they may represent a diagnostic, ethical, and philosophical dilemma because their significance is unclear. While some coincidental findings may lead to beneficial diagnoses, others may lead to overdiagnosis that results in unnecessary testing and treatment, sometimes called the "cascade effect".
Radiology (X-rays) is used in the diagnosis of tuberculosis. Abnormalities on chest radiographs may be suggestive of, but are never diagnostic of TB, but can be used to rule out pulmonary TB.

Atelectasis is the partial collapse or closure of a lung resulting in reduced or absence in gas exchange. It is usually unilateral, affecting part or all of one lung. It is a condition where the alveoli are deflated down to little or no volume, as distinct from pulmonary consolidation, in which they are filled with liquid. It is often referred to informally as a collapsed lung, although more accurately it usually involves only a partial collapse, and that ambiguous term is also informally used for a fully collapsed lung caused by a pneumothorax.

Scimitar syndrome, or congenital pulmonary venolobar syndrome, is a rare congenital heart defect characterized by anomalous venous return from the right lung. This anomalous pulmonary venous return can be either partial (PAPVR) or total (TAPVR). The syndrome associated with PAPVR is more commonly known as Scimitar syndrome after the curvilinear pattern created on a chest radiograph by the pulmonary veins that drain to the inferior vena cava. This radiographic density often has the shape of a scimitar, a type of curved sword. The syndrome was first described by Catherine Neill in 1960.

A bronchopulmonary segment is a portion of lung supplied by a specific segmental bronchus and its vessels. These arteries branch from the pulmonary and bronchial arteries, and run together through the center of the segment. Veins and lymphatic vessels drain along the edges of the segment. The segments are separated from each other by layers of connective tissue that forms them into discrete anatomical and functional units. This separation means that a bronchopulmonary segment can be surgically removed without affecting the function of the others.

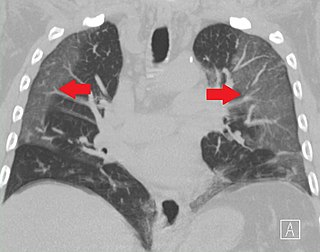
In radiology, the tree-in-bud sign is a finding on a CT scan that indicates some degree of airway obstruction. The tree-in-bud sign is a nonspecific imaging finding that implies impaction within bronchioles, the smallest airway passages in the lung. The differential for this finding includes malignant and inflammatory etiologies, either infectious or sterile. This includes fungal infections, mycobacterial infections such as tuberculosis or mycobacterium avium intracellulare, bronchopneumonia, chronic aspiration pneumonia, cystic fibrosis or cellular impaction from bronchovascular spread of malignancy, as can occur with breast cancer, leukemia or lymphoma. It also includes lung manifestations of autoimmune diseases such as Sjögren syndrome or rheumatoid arthritis.
Williams–Campbell syndrome (WCS) is a disease of the airways where cartilage in the bronchi is defective. It is a form of congenital cystic bronchiectasis. This leads to collapse of the airways and bronchiectasis. It acts as one of the differential to allergic bronchopulmonary aspergillosis. WCS is a deficiency of the bronchial cartilage distally.

A lung nodule or pulmonary nodule is a relatively small focal density in the lung. A solitary pulmonary nodule (SPN) or coin lesion, is a mass in the lung smaller than three centimeters in diameter. A pulmonary micronodule has a diameter of less than three millimetres. There may also be multiple nodules.

Respiratory bronchiolitis is a lung disease associated with tobacco smoking. In pathology, it is defined by the presence of "smoker's macrophages". When manifesting significant clinical symptoms it is referred to as respiratory bronchiolitis interstitial lung disease (RB-ILD).

In human anatomy, an azygos lobe is a normal anatomical variation of the upper lobe of the right lung. It is seen in 0.3% of the population. Embryologically, it arises from an anomalous lateral course of the azygos vein, in a pleural septum within the apical segment of the right upper lobe or in other words an azygos lobe is formed when the right posterior cardinal vein, one of the precursors of the azygos vein, fails to migrate over the apex of the lung and penetrates it instead, carrying along two pleural layers as the azygous fissure, that invaginates into the upper portion of the right upper lobe.
In radiology, the Golden S sign, also known as the S sign of Golden, is a radiologic sign seen on chest X-ray that suggests a central lung mass or a lung collapse. It was first described by, and subsequently named after, Dr Ross Golden (1889–1975) in 1925 in association with bronchial carcinoma, but it is also seen in metastatic cancer, enlarged lymph nodes, and collapse of the right upper lobe of the lung.
Ground-glass opacity (GGO) is a finding seen on chest x-ray (radiograph) or computed tomography (CT) imaging of the lungs. It is typically defined as an area of hazy opacification (x-ray) or increased attenuation (CT) due to air displacement by fluid, airway collapse, fibrosis, or a neoplastic process. When a substance other than air fills an area of the lung it increases that area's density. On both x-ray and CT, this appears more grey or hazy as opposed to the normally dark-appearing lungs. Although it can sometimes be seen in normal lungs, common pathologic causes include infections, interstitial lung disease, and pulmonary edema.
Radiation lobectomy is a form of radiation therapy used in interventional radiology to treat liver cancer. It is performed in patients that would be surgical candidates for resection, but cannot undergo surgery due to insufficient remaining liver tissue. It consists of injecting small radioactive beads loaded with yttrium-90 into the hepatic artery feeding the hepatic lobe in which the tumor is located. This is done with the intent of inducing growth in the contralateral hepatic lobe, not dissimilarly from portal vein embolization (PVE).
Fleischner sign is a radiological sign that aids the diagnosis of pulmonary embolism. The sign indicates the dilatation of the proximal pulmonary arteries due to pulmonary embolism. It was named after Felix Fleischner, who first described it. The Fleishner sign is seen both on X-ray and CT scan of chest/thorax.

Collateral ventilation is a back-up system of alveolar ventilation that can bypass the normal route of airflow when airways are restricted or obstructed. The pathways involved include those between adjacent alveoli, between bronchioles and alveoli, and those between bronchioles . Collateral ventilation also serves to modulate imbalances in ventilation and perfusion a feature of many diseases. The pathways are altered in lung diseases particularly asthma, and emphysema. A similar functional pattern of collateralisation is seen in the circulatory system of the heart.

Lung surgery is a type of thoracic surgery involving the repair or removal of lung tissue, and can be used to treat a variety of conditions ranging from lung cancer to pulmonary hypertension. Common operations include anatomic and nonanatomic resections, pleurodesis and lung transplants. Though records of lung surgery date back to the Classical Age, new techniques such as VATS continue to be developed.
The black pleura sign is a radiological feature observed in pulmonary alveolar microlithiasis (PAM), a rare lung disorder characterized by the accumulation of tiny calcium phosphate deposits, known as microliths, within the alveoli. This sign appears as a thin, dark (lucent) line beneath the ribs on imaging studies, contrasting with the diffusely dense, calcified lung parenchyma.
References
- ↑ Kattan, K. R.; Eyler, W. R.; Felson, B. (March 1980). "The juxtaphrenic peak in upper lobe collapse". Radiology. 134 (3): 763–765. doi:10.1148/radiology.134.3.7355230. ISSN 0033-8419. PMID 7355230 . Retrieved 14 July 2021.
- 1 2 Kumaresh, Athiyappan; Kumar, Mitesh; Dev, Bhawna; Gorantla, Rajani; Sai, PM Venkata; Thanasekaraan, Vijayalakshmi (31 July 2015). "Back to Basics – 'Must Know' Classical Signs in Thoracic Radiology". Journal of Clinical Imaging Science. 5: 43. doi: 10.4103/2156-7514.161977 . ISSN 2156-7514. PMC 4541161 . PMID 26312141.
- ↑ Cameron, D. C. (November 1993). "The juxtaphrenic peak (Katten's sign) is produced by rotation of an inferior accessory fissure". Australasian Radiology. 37 (4): 332–335. doi:10.1111/j.1440-1673.1993.tb00091.x. ISSN 0004-8461. PMID 8257331 . Retrieved 14 July 2021.
- ↑ Davis, S. D.; Yankelevitz, D. F.; Wand, A.; Chiarella, D. A. (January 1996). "Juxtaphrenic peak in upper and middle lobe volume loss: assessment with CT". Radiology. 198 (1): 143–149. doi:10.1148/radiology.198.1.8539368. PMID 8539368.
- ↑ Konen, E.; Rozenman, J.; Simansky, D. A.; Yellin, A.; Greenberg, I.; Konen, O.; Hertz, M.; Itzchak, Y. (October 2001). "Prevalence of the juxtaphrenic peak after upper lobectomy". AJR. American Journal of Roentgenology. 177 (4): 869–873. doi:10.2214/ajr.177.4.1770869. ISSN 0361-803X. PMID 11566691 . Retrieved 14 July 2021.