Palliative care is an interdisciplinary medical caregiving approach aimed at optimizing quality of life and mitigating suffering among people with serious, complex, and often terminal illnesses. Within the published literature, many definitions of palliative care exist. The World Health Organization (WHO) describes palliative care as "an approach that improves the quality of life of patients and their families facing the problems associated with life-threatening illness, through the prevention and relief of suffering by means of early identification and impeccable assessment and treatment of pain and other problems, physical, psychosocial, and spiritual". In the past, palliative care was a disease specific approach, but today the WHO takes a broader patient-centered approach that suggests that the principles of palliative care should be applied as early as possible to any chronic and ultimately fatal illness. This shift was important because if a disease-oriented approach is followed, the needs and preferences of the patient are not fully met and aspects of care, such as pain, quality of life, and social support, as well as spiritual and emotional needs, fail to be addressed. Rather, a patient-centered model prioritizes relief of suffering and tailors care to increase the quality of life for terminally ill patients.
Terminal illness or end-stage disease is a disease that cannot be cured or adequately treated and is expected to result in the death of the patient. This term is more commonly used for progressive diseases such as cancer, dementia or advanced heart disease than for injury. In popular use, it indicates a disease that will progress until death with near absolute certainty, regardless of treatment. A patient who has such an illness may be referred to as a terminal patient, terminally ill or simply as being terminal. There is no standardized life expectancy for a patient to be considered terminal, although it is generally months or less. Life expectancy for terminal patients is a rough estimate given by the physician based on previous data and does not always reflect true longevity. An illness which is lifelong but not fatal is a chronic condition.
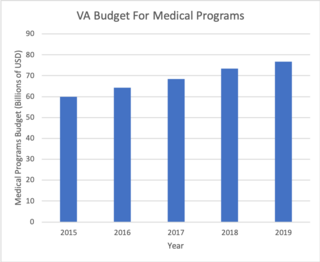
The Veterans Health Administration (VHA) is the component of the United States Department of Veterans Affairs (VA) led by the Under Secretary of Veterans Affairs for Health that implements the healthcare program of the VA through a nationalized healthcare service in the United States, providing healthcare and healthcare-adjacent services to veterans through the administration and operation of 146 VA Medical Centers (VAMC) with integrated outpatient clinics, 772 Community Based Outpatient Clinics (CBOC), and 134 VA Community Living Centers Programs. It is the largest division in the department, and second largest in the entire federal government, employing over 350,000 employees. All VA hospitals, clinics and medical centers are owned by and operated by the Department of Veterans Affairs, and all of the staff employed in VA hospitals are federal employees. Because of this, veterans that qualify for VHA healthcare do not pay premiums or deductibles for their healthcare but may have to make copayments depending on the medical procedure. VHA is not a part of the US Department of Defense Military Health System.
The term managed care or managed healthcare is used in the United States to describe a group of activities intended to reduce the cost of providing health care and providing American health insurance while improving the quality of that care. It has become the predominant system of delivering and receiving American health care since its implementation in the early 1980s, and has been largely unaffected by the Affordable Care Act of 2010.
...intended to reduce unnecessary health care costs through a variety of mechanisms, including: economic incentives for physicians and patients to select less costly forms of care; programs for reviewing the medical necessity of specific services; increased beneficiary cost sharing; controls on inpatient admissions and lengths of stay; the establishment of cost-sharing incentives for outpatient surgery; selective contracting with health care providers; and the intensive management of high-cost health care cases. The programs may be provided in a variety of settings, such as Health Maintenance Organizations and Preferred Provider Organizations.
A pain scale measures a patient's pain intensity or other features. Pain scales are a common communication tool in medical contexts, and are used in a variety of medical settings. Pain scales are a necessity to assist with better assessment of pain and patient screening. Pain measurements help determine the severity, type, and duration of the pain, and are used to make an accurate diagnosis, determine a treatment plan, and evaluate the effectiveness of treatment. Accurately measuring pain is a necessity in medical settings, especially if the pain measurement is going to be used as a screening tool, either for potential diseases or medical problems, or as a type of triage to determine urgency of one patient over another. Pain scales are based on trust, cartoons (behavioral), or imaginary data, and are available for neonates, infants, children, adolescents, adults, seniors, and persons whose communication is impaired. Pain assessments are often regarded as "the 5th vital sign".
In the healthcare industry, pay for performance (P4P), also known as "value-based purchasing", is a payment model that offers financial incentives to physicians, hospitals, medical groups, and other healthcare providers for meeting certain performance measures. Clinical outcomes, such as longer survival, are difficult to measure, so pay for performance systems usually evaluate process quality and efficiency, such as measuring blood pressure, lowering blood pressure, or counseling patients to stop smoking. This model also penalizes health care providers for poor outcomes, medical errors, or increased costs. Integrated delivery systems where insurers and providers share in the cost are intended to help align incentives for value-based care.
Patient safety is a discipline that emphasizes safety in health care through the prevention, reduction, reporting and analysis of error and other types of unnecessary harm that often lead to adverse patient events. The frequency and magnitude of avoidable adverse events, often known as patient safety incidents, experienced by patients was not well known until the 1990s, when multiple countries reported significant numbers of patients harmed and killed by medical errors. Recognizing that healthcare errors impact 1 in every 10 patients around the world, the World Health Organization (WHO) calls patient safety an endemic concern. Indeed, patient safety has emerged as a distinct healthcare discipline supported by an immature yet developing scientific framework. There is a significant transdisciplinary body of theoretical and research literature that informs the science of patient safety with mobile health apps being a growing area of research.
A Patient Safety Organization (PSO) is a group, institution, or association that improves medical care by reducing medical errors. Common functions of patient safety organizations are data collection, analysis, reporting, education, funding, and advocacy. A PSO differs from a Federally designed Patient Safety Organization (PSO), which provides health care providers in the U.S. privilege and confidentiality protections for efforts to improve patient safety and the quality of patient care delivery

Charles N. ("Chip") Kahn III is the president and chief executive officer of the Federation of American Hospitals (FAH), whose member companies own nearly 20 percent of all American hospital beds. Kahn and the FAH represent their members on health policy issues like health care reform and hospital care quality improvement.
End-of-life care (EOLC) refers to health care provided in the time leading up to a person's death. End-of-life care can be provided in the hours, days, or months before a person dies and encompasses care and support for a person's mental and emotional needs, physical comfort, spiritual needs, and practical tasks.
A never event is the "kind of mistake that should never happen" in the field of medical treatment. According to the Leapfrog Group never events are defined as "adverse events that are serious, largely preventable, and of concern to both the public and health care providers for the purpose of public accountability."
Health information technology (HIT) is health technology, particularly information technology, applied to health and health care. It supports health information management across computerized systems and the secure exchange of health information between consumers, providers, payers, and quality monitors. Based on a 2008 report on a small series of studies conducted at four sites that provide ambulatory care – three U.S. medical centers and one in the Netherlands, the use of electronic health records (EHRs) was viewed as the most promising tool for improving the overall quality, safety and efficiency of the health delivery system.

In general, quality of life is the perceived quality of an individual's daily life, that is, an assessment of their well-being or lack thereof. This includes all emotional, social and physical aspects of the individual's life. In health care, health-related quality of life (HRQoL) is an assessment of how the individual's well-being may be affected over time by a disease, disability or disorder.
Diane E. Meier, an American geriatrician and palliative care specialist. In 1999, Dr. Meier founded the Center to Advance Palliative Care, a national organization devoted to increasing access to quality health care in the United States for people living with serious illness. She continues to serve as CAPC's Director Emerita and Strategic Medical Advisor. Meier is also Vice-Chair for Public Policy, Professor of Geriatrics and Palliative Medicine and Catherine Gaisman Professor of Medical Ethics at the Icahn School of Medicine at Mount Sinai Hospital in New York City. Meier was founder and Director of the Hertzberg Palliative Care Institute at the Icahn School of Medicine in New York City from 1997 to 2011.
POLST is an approach to improving end-of-life care in the United States, encouraging providers to speak with the severely ill and create specific medical orders to be honored by health care workers during a medical crisis. POLST began in Oregon in 1991 and currently exists in 46 states; some of the 46 states have the program in development. The POLST document is a standardized, portable, brightly colored single page medical order that documents a conversation between a provider and an individual with a serious illness or frailty towards the end of life. A POLST form allows emergency medical services to provide treatment that the individual prefers before possibly transporting to an emergency facility.

The Pennsylvania Health Care Quality Alliance (PHCQA) is a nonprofit group of healthcare organizations, including the Hospital and Healthsystem Association of Pennsylvania, which represents more than 225 hospitals and health systems across Pennsylvania in the United States.
Health care quality is a level of value provided by any health care resource, as determined by some measurement. As with quality in other fields, it is an assessment of whether something is good enough and whether it is suitable for its purpose. The goal of health care is to provide medical resources of high quality to all who need them; that is, to ensure good quality of life, cure illnesses when possible, to extend life expectancy, and so on. Researchers use a variety of quality measures to attempt to determine health care quality, including counts of a therapy's reduction or lessening of diseases identified by medical diagnosis, a decrease in the number of risk factors which people have following preventive care, or a survey of health indicators in a population who are accessing certain kinds of care.
The teach-back method, also called the "show-me" method, is a communication confirmation method used by healthcare providers to confirm whether a patient understands what is being explained to them. If a patient understands, they are able to "teach-back" the information accurately. This is a communication method intended to improve health literacy.
The role of spirituality in health care has received significant research attention due to its benefits for patients and health care professionals. Integrating spirituality in healthcare can enhance healthcare professionals' ability to communicate effectively with patients and families. It can also have a positive impact on the health and well-being of patients due to its potential to enhance patients' ability to cope with illness and achieve better physical and mental health outcomes. As per 2014, more than 70 medical schools in the United States offer courses on spirituality and medicine. The Association of American Medical Colleges has co-sponsored, with the National Institute for Healthcare Research, four conferences, on curricular development in spirituality and medicine since 1997.
Value-based health care (VBHC) is a framework for restructuring health care systems with the overarching goal of value for patients, with value defined as health outcomes per unit of costs. The concept was introduced in 2006 by Michael Porter and Elizabeth Olmsted Teisberg, though implementation efforts on aspects of value-based care began long before then in the 1990s. With patient value as the overarching goal, VBHC emphasis systematic measurement of outcomes and costs, restructuring provider organizations, and transitioning toward bundled payments. Within this framework, cost reduction alone is not seen as proper strategy for healthcare systems: health outcomes have to improve to enhance value. Although value-based health care is seen as a priority in many health systems worldwide, a global assessment in 2016 found many countries are only beginning to align their health systems with VBHC-principles. Additionally, several studies report incoherent implementation efforts, and there seem to be various interpretations of VBHC, both within and across countries.